Fact file by Neil FrancisPosted on Thursday 10th September 2020 at 11:27pm
World-first report of VAD use amongst minors is now available for download.
Differences of opinion continue to be expressed regarding law reform to permit voluntary assisted dying (VAD) for minors: persons under the age of legal majority or adulthood, which in most jurisdictions is 18 years. Some claims are florid and ill-informed. To date, no cohesive report has been published regarding the actual use of VAD by minors in jurisdictions where it is lawful. This research aims to address that shortfall.
This study examines official evidence from lawful jurisdictions regarding the extent and nature of VAD amongst minors. Its aim is to facilitate calmer public discourse and more fully inform legislators considering VAD law reform proposals.
Findings
VAD is currently a lawful choice for minors in the Netherlands, Belgium, Switzerland and Colombia.
Dutch and Belgian legislation, and Colombian regulations, stipulate additional requirements regarding minors.
Available Dutch and Belgian data reveal very low rates of use, between zero and three cases per annum, with parental involvement in decision making.
There are no cases of VAD amongst minors on record in Switzerland.
No official case data is available from Colombia. However, given the extremely low rate of VAD use overall, cases amongst minors are highly unlikely.
While use of VAD laws by minors is rare, a review of case records reveals — as for adults — severe refractory underlying illness with extreme, unrelievable suffering.
Conclusions
Use of VAD by minors in lawful jurisdictions is rare, but nevertheless occurs with parental involvement in decision making, and otherwise as for adults: in cases of severe, refractory underlying illness with extreme, unrelievable suffering.
Fact file by Neil FrancisPosted on Sunday 13th November 2016 at 1:47am
Assisted dying rates in Dutch-speaking cultures (orange bars) are much higher than elsewhere.
In this whitepaper, Benelux (Belgium, Netherlands and Luxembourg) primary empirical data on assisted dying is analysed — including with new and advanced approaches — to provide fresh insights into contemporary practices. Investigation reveals that the assisted dying rate in Dutch-speaking cultures appears to be uniquely higher than in other cultures irrespective of the permissiveness of the legislative framework, yet is still practiced conservatively.
Download a full copy of the Whitepaper here: PDF (648Kb).
Summary
This new compilation and unique analysis of primary research data from statutory authorities and the peer-reviewed literature provides fresh insights into assisted dying practice in Benelux, including:
Rates of assisted dying in the Netherlands and Belgium have followed an expected sigmoid curve, now beginning to level out.
Several factors have contributed to the higher increase in the Netherlands rate, including recovery from a suppression of cases immediately following statutory reform, a rise in cancer diagnoses, and an increase in granting of assisted dying through new visiting teams launched in 2012.
Both Netherlands and Belgium doctors demonstrate caution if not conservatism when assessing assisted dying requests.
Despite most assisted dying occurring in cases of cancer, fewer than one in ten cancer deaths in the Netherlands and one in twenty in Belgium is an assisted death.
Other conditions such as degenerative neurological, pulmonary and circulatory illnesses each account for a very small proportion of the increase in cases since legalisation in Benelux.
The assisted dying rate in dementia and other mental illness is very low despite controversy around—and a tiny rise in granting of—such cases.
The hypothesis that females or the elderly would be ‘vulnerable’ to assisted dying law is contradicted by the data.
The rate of non-voluntary euthanasia has decreased significantly in both the Netherlands and Belgium since assisted dying was permitted by statute.
Assisted dying rates in Dutch-speaking cultures are significantly higher than in non-Dutch cultures, seemingly unrelated to the permissiveness of the jurisdiction’s legal framework.
Benelux country reported assisted dying rates (as a percentage of all deaths)
as at 2014. The three countries have similar assisted dying laws.
Fact file by Neil FrancisPosted on Thursday 7th July 2016 at 10:19pm
Lead author Professor Ezekiel Emanuel discusses the findings of the JAMA study.
Several of the world's foremost researchers in medical end-of-life matters have released a detailed and comprehensive review of the practice of assisted dying in lawful jurisdictions around the world. Published in the Journal of the American Medical Association, it does not support slippery slope hypotheses.
Professors from universities in the USA, the Netherlands and Belgium studied data from government and statutory authority reports, primary scientific studies and other sources to examine how assisted dying has been practiced in different jurisdictions around the world where it is lawful in one form or another: self-administered medication (physician-assisted dying) or physician-administered medication (active voluntary euthanasia).1
Their primary conclusion is that:
"Euthanasia and physician-assisted suicide are increasingly being legalized, remain relatively rare, and primarily involve patients with cancer. Existing data do not indicate widespread abuse of these practices."
Key findings
Key findings include:
Public opinion favouring assisted dying in developed countries has been increasing, or remained stable at high levels of approval.
The trends seem to correlate with decreasing religiosity in Western countries.
The only place where assisted dying approval appears to be decreasing is in eastern Europe, where religiosity has been increasing.
Approval amongst physicians seems to be consistently lower than amongst the public.
Assisted dying occurs everywhere, including juridictions where it is unlawful (as I have previously reported).
Most individuals who choose assisted dying have advanced cancer (as I have previously reported).
Supposedly 'vulnerable' groups are not represented in assisted dying figures at rates any higher than their presence in the overall population.
Numbers of assisted deaths in lawful jurisdictions continue to increase, but represent a tiny minority of deaths.
In jurisdictions where only self-administration is permitted, assisted deaths represent around 0.3% of all deaths.
In jurisdictions where physicians may administer, assisted deaths represent around 3–5% of all deaths.
Assisted deaths for minors and those with dementia are a very small minority of cases (as I have previously reported).
The dominant reasons for requesting assisted death include loss of autonomy and dignity and the inability to enjoy life and regular activities; not physical pain.
Doctors still report that honouring a request for assisted death is emotionally burdensome; not a routine or welcomed option.
"In no jurisdiction was there evidence that vulnerable patients have been receiving euthanasia or physician-assisted suicide at rates higher than those in the general population."
Complication rates
One aspect of the study is worthy of special mention: the small rate of assisted dying procedure complications. The available data suggests that complications may occur more often for self-administered medication than for physician administration:
For self-administration—
Difficulty in swallowing in 9.6% of cases
Vomiting or seizures in 8.8% of cases
Awakening from coma in 12.3% of cases
For physician administration—
Technical problems such as difficulty in finding a suitable vein in 4.5% of cases
Vomiting or seizures in 3.7% of cases
Awakening from coma in 0.9% of cases
This data is however of Dutch practice in the 1990s, before assisted dying was codified in statute—at a time when practice was poorly defined and a range of drugs, including opioids, were widely used. Now, practice is well-defined with almost universal use of barbiturates. The researchers expressly note that these complication rates may well have reduced.
Further, the authors refer to more recent data from Oregon and Washington which indicate very much lower complication rates (in those jurisdictions for self-administration only):
In Oregon, the complication rates are around 2.4% for regurgitation and 0.7% for awakening from coma.
In Washington, the complication rates are around 1.4% for regurgitation, plus a single case of seizure.
The importance of context
It is worth comparing the complication rates of assisted dying procedures with rates for other medical interventions to provide an appropriate context so that they may be realistically interpreted.
For example, a study of common over-the-counter analgesics for short-term pain management2 found that significant adverse effects occurred amongst 13.7% of ibuprofen users, 14.5% of paracetamol useres and 18.7% of aspirin users.
In another example, an anlaysis of primary research about surgical outcomes found that 14.4% had adverse events, almost half of which (47.5%) were moderate to fatal in severity.3
Conclusion
The study is a solid synthesis of research data and indicates that assisted dying is accessed sparingly and in accordance with the intentions of each legislature.
The adverse event rate for assisted dying appears to be substantially lower than the rate of adverse events in the use of common over-the-counter analgesics and in surgery.
References
Emanuel, EJ, Onwuteaka-Philipsen, BD, Urwin, JW & Cohen, J 2016, 'Attitudes and practices of euthanasia and physician-assisted suicide in the united states, canada, and europe', JAMA, 316(1), pp. 79-90.
Moore, N, Ganse, EV, Parc, J-ML, Wall, R, Schneid, H, Farhan, M, Verrière, F & Pelen, F 1999, 'The PAIN Study: Paracetamol, Aspirin and Ibuprofen new tolerability study', Clinical Drug Investigation, 18(2), pp. 89-98.
Anderson, O, Davis, R, Hanna, GB & Vincent, CA 2013, 'Surgical adverse events: a systematic review', Am J Surg, 206(2), pp. 253-62.
Fact file by Neil FrancisPosted on Thursday 28th January 2016 at 1:30am
Around the world, doctors help patients with assisted dying, regardless of whether it is legal in their jurisdiction or not.
For example, in Australia, where assisted dying is illegal, research reveals that assisted dying is widely practiced. Many Australian nurses have collaborated with doctors to provide assisted dying, and have occasionally even done so without consulting a doctor (Kuhse & Singer 1993). Nurses in New Zealand also provide assisted dying, sometimes without consulting a doctor (Malpas, Mitchell & Koschwanez 2015; Mitchell & Owens 2004).
"Euthanasia is common. It's practiced out of sight, under wraps, no regulation, no rules, no supervision." Prof. Peter Baum (Baum 2001)
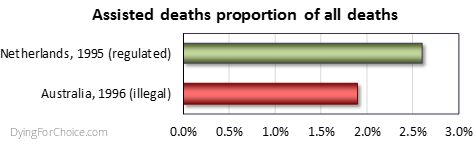
Professor Baum's statement is borne out by scientific research. A national survey of Australian doctors in 1996 found that 1.9% of deaths were the result of voluntary euthanasia (VE) or physician-assisted dying (PAD) (Kuhse et al. 1997). By comparison, the rate in the Netherlands in 1995 (the closest year of empirical research data) was 2.6% (Onwuteaka-Philipsen et al 2012). The rate of medically assisted deaths in Australia, where the practice is illegal, was three quarters the rate of the Netherlands, where the practice is legal.
Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.
Forms of medically assisted dying have been found to occur not only in Australia (and in the Netherlands where it has been lawful for decades), but in Belgium prior to its law reform (Chambaere et al. 2015); Switzerland, Denmark, Sweden and Italy (van der Heide et al. 2003); the UK (Seale 2009a; Seale 2009b); the USA (Back et al. 1996; Bonn 2000; Emanuel, Fairclough & Clarridge 1996; Lachman 2010; Schwarz 2003; Schwarz 2004); France (Riou et al. 2015); Norway (Forde & Aasland 2014; Forde, Aasland & Falkum 1997); and even in conservative Greece (Voultsos, Njau & Vlachou 2010); Northern Ireland (McGlade 2000) and Pakistan (Imran et al. 2014).
Indeed, "euthanasia is performed worldwide, regardless of the existence of laws governing it" (Gastmans et al. 2006), "in all countries studied" (Muller, Kimsma & Van Der Wal 1998), "albeit in a secretive manner" (Rosenfeld 2000), "in the privacy of their [doctor-patient] relationship" (Cassell 1995), with repeated involvement of some physicians (Smith 2007), and frequent failure to adhere to high standards when illegal (Emanuel et al 1998).
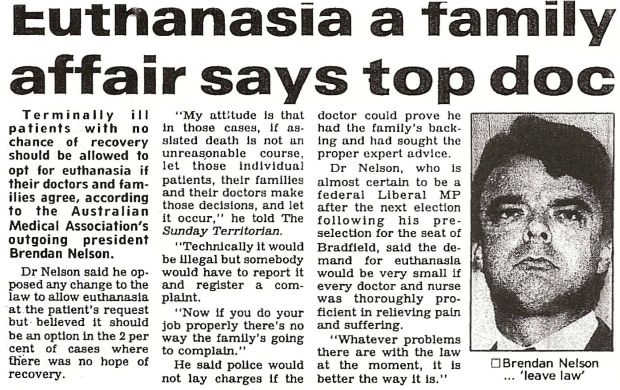
Even Dr Brendan Nelson, while President of the Australian Medical Association, acknowledged that he had helped hasten the death of a patient. He stated that in the "2 percent of cases" where there was no hope of recovery, that "patients, their families and their doctors make those decisions [for euthanasia]" though clandestinely, because "technically it would be illegal" (Nelson 1995).
AMA's President, Brendan Nelson, in 1995.
The evidence is irrefutable: there is underground assisted dying worldwide and it demonstrates that there is a profound need for assisted dying law reform to allow dying patients the right to seek a peaceful hastened death, and to protect doctors and nurses who provide that assistance. Law reform would also force assisted dying from the dark shadows, creating transparency and accountability around the process, which would then be open to discussion and improvement if required.
Intolerable and unrelievable patient suffering drives underground assisted dying across the world in jurisdictions where it is illegal, with no standards of practice or transparent oversight.
References
Back, AL, Wallace, JI, Starks, HE & Pearlman, RA 1996, 'Physician-assisted suicide and euthanasia in Washington State: Patient requests and physician responses', JAMA, vol. 275, no. 12, pp. 919-925.
Baum, P 2001, ABC News, TV broadcast 23 Jan, ABC, Sydney.
Bonn, D 2000, 'Support for euthanasia falls as care of dying patients improves', The Lancet Oncology, vol. 1, no. 3, p. 133.
Cassell, EJ 1995, 'Treating the patient's subjective state', Pain Forum, vol. 4, no. 3, pp. 186-188.
Chambaere, K, Vander Stichele, R, Mortier, F, Cohen, J & Deliens, L 2015, 'Recent trends in euthanasia and other end-of-life practices in Belgium', N Engl J Med, vol. 372, no. 12, pp. 1179-1181.
Douglas, C, Kerridge, IH, Rainbird, KJ, McPhee, JR, Hancock, L & Spigelman, AD 2001, 'The intention to hasten death: a survey of attitudes and practices of surgeons in Australia', Medical Journal of Australia, vol. 175, no. 10, pp. 511-515.
Emanuel, EJ, Daniels, ER, Fairclough, DL & Clarridge, BR 1998, 'The practice of euthanasia and physician-assisted suicide in the United States: adherence to proposed safeguards and effects on physicians', JAMA, vol. 280, no. 6, pp. 507-513.
Emanuel, EJ, Fairclough, DL & Clarridge, BR 1996, 'Euthanasia and physician-assisted suicide: Attitudes and experiences of oncology patients, oncologists, and the public', Lancet, vol. 347, no. 9018, pp. 1805-1810.
Forde, R & Aasland, OG 2014, 'Are end-of-life practices in Norway in line with ethics and law?', Acta Anaesthesiol Scand, Aug 14.
Forde, R, Aasland, OG & Falkum, E 1997, 'The ethics of euthanasia -- attitude and practice maong Norwegian physicians', Social Science & Medicine, vol. 45, no. 6, pp. 887-982.
Gastmans, C, Lemiengre, J, van der Wal, G, Schotsmans, P & Dierckx de Casterle, B 2006, 'Prevalence and content of written ethics policies on euthanasia in Catholic healthcare institutions in Belgium (Flanders)', Health Policy, vol. 76, no. 2, pp. 169-78.
Imran, N, Haider, II, Jawaid, M & Mazhar, N 2014, 'Health ethics education: Knowledge, attitudes and practice of healthcare ethics among interns and residents in Pakistan', Journal of Postgraduate Medical Institute, vol. 28, no. 4, pp. 383-389.
Kuhse, H & Singer, P 1993, 'Voluntary euthanasia and the nurse: an Australian survey', International Journal of Nursing Studies, vol. 30, no. 4, pp. 311-322.
Kuhse, H, Singer, P, Baume, P, Clark, M & Rickard, M 1997, 'End-of-life decisions in Australian medical practice', Medical Journal of Australia, vol. 166, no. 4, pp. 191-196.
Lachman, V 2010, 'Physician-assisted suicide: compassionate liberation or murder?', Medsurg nursing : official journal of the Academy of Medical-Surgical Nurses, vol. 19, no. 2, pp. 121-125.
Malpas, P, Mitchell, K & Koschwanez, H 2015, 'End-of-life medical decision making in general practice in New Zealand—13 years on', New Zealand Medical Journal, vol. 128, no. 1418, pp. 27-39.
McGlade, KJ, Slaney, L, Bunting, BP & Gallagher, AG 2000, 'Voluntary euthanasia in Northern Ireland: General practitioners' beliefs, experiences, and actions', British Journal of General Practice, vol. 50, no. 459, pp. 794-797.
Mitchell, K & Owens, G 2004, 'End of life decision-making by New Zealand general practitioners: A national survey', New Zealand Medical Journal, vol. 117, no. 1196, pp. 1-11.
Muller, MT, Kimsma, GK & Van Der Wal, G 1998, 'Euthanasia and assisted suicide: Facts, figures and fancies with special regard to old age', Drugs and Aging, vol. 13, no. 3, pp. 185-191.
Nelson, B 1995, 'Euthanasia a family affair says top doc', The Sunday Territorian, Darwin, 21 May.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Riou, F, Aubry, R, Pontone, S & Pennec, S 2015, 'When physicians report having used medical drugs to deliberately end a patient's life: Findings of the "end-of-life in France" survey', Journal of Pain and Symptom Management, vol. 50, no. 2, pp. 208-215.
Rosenfeld, B 2000, 'Assisted suicide, depression, and the right to die', Psychology, Public Policy, and Law, vol. 6, no. 2, pp. 467-488.
Schwarz, JK 2003, 'Understanding and responding to patients' requests for assistance in dying', Journal of Nursing Scholarship, vol. 35, no. 4, pp. 377-384.
Schwarz, JK 2004, 'Responding to persistent requests for assistance in dying: a phenomenological inquiry', International Journal of Palliative Nursing, vol. 10, no. 5, pp. 225-235.
Seale, C 2009a, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, vol. 23, no. 3, pp. 198-204.
Seale, C 2009b, 'Hastening death in end-of-life care: a survey of doctors', Social Science & Medicine, vol. 69, no. 11, pp. 1659-1666.
Smith, SW 2007, 'Some realism about end of life: The current prohibition and the euthanasia underground', American Journal of Law and Medicine, vol. 33, no. 1, pp. 55-95.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, vol. 362, no. 9381, pp. 345-350.
Voultsos, P, Njau, SN & Vlachou, M 2010, 'The issue of euthanasia in Greece from a legal viewpoint', J Forensic Leg Med, vol. 17, no. 3, pp. 131-6.

 Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.
Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.