Fact file by Neil FrancisPosted on Thursday 7th July 2016 at 10:19pm
Lead author Professor Ezekiel Emanuel discusses the findings of the JAMA study.
Several of the world's foremost researchers in medical end-of-life matters have released a detailed and comprehensive review of the practice of assisted dying in lawful jurisdictions around the world. Published in the Journal of the American Medical Association, it does not support slippery slope hypotheses.
Professors from universities in the USA, the Netherlands and Belgium studied data from government and statutory authority reports, primary scientific studies and other sources to examine how assisted dying has been practiced in different jurisdictions around the world where it is lawful in one form or another: self-administered medication (physician-assisted dying) or physician-administered medication (active voluntary euthanasia).1
Their primary conclusion is that:
"Euthanasia and physician-assisted suicide are increasingly being legalized, remain relatively rare, and primarily involve patients with cancer. Existing data do not indicate widespread abuse of these practices."
Key findings
Key findings include:
Public opinion favouring assisted dying in developed countries has been increasing, or remained stable at high levels of approval.
The trends seem to correlate with decreasing religiosity in Western countries.
The only place where assisted dying approval appears to be decreasing is in eastern Europe, where religiosity has been increasing.
Approval amongst physicians seems to be consistently lower than amongst the public.
Assisted dying occurs everywhere, including juridictions where it is unlawful (as I have previously reported).
Most individuals who choose assisted dying have advanced cancer (as I have previously reported).
Supposedly 'vulnerable' groups are not represented in assisted dying figures at rates any higher than their presence in the overall population.
Numbers of assisted deaths in lawful jurisdictions continue to increase, but represent a tiny minority of deaths.
In jurisdictions where only self-administration is permitted, assisted deaths represent around 0.3% of all deaths.
In jurisdictions where physicians may administer, assisted deaths represent around 3–5% of all deaths.
Assisted deaths for minors and those with dementia are a very small minority of cases (as I have previously reported).
The dominant reasons for requesting assisted death include loss of autonomy and dignity and the inability to enjoy life and regular activities; not physical pain.
Doctors still report that honouring a request for assisted death is emotionally burdensome; not a routine or welcomed option.
"In no jurisdiction was there evidence that vulnerable patients have been receiving euthanasia or physician-assisted suicide at rates higher than those in the general population."
Complication rates
One aspect of the study is worthy of special mention: the small rate of assisted dying procedure complications. The available data suggests that complications may occur more often for self-administered medication than for physician administration:
For self-administration—
Difficulty in swallowing in 9.6% of cases
Vomiting or seizures in 8.8% of cases
Awakening from coma in 12.3% of cases
For physician administration—
Technical problems such as difficulty in finding a suitable vein in 4.5% of cases
Vomiting or seizures in 3.7% of cases
Awakening from coma in 0.9% of cases
This data is however of Dutch practice in the 1990s, before assisted dying was codified in statute—at a time when practice was poorly defined and a range of drugs, including opioids, were widely used. Now, practice is well-defined with almost universal use of barbiturates. The researchers expressly note that these complication rates may well have reduced.
Further, the authors refer to more recent data from Oregon and Washington which indicate very much lower complication rates (in those jurisdictions for self-administration only):
In Oregon, the complication rates are around 2.4% for regurgitation and 0.7% for awakening from coma.
In Washington, the complication rates are around 1.4% for regurgitation, plus a single case of seizure.
The importance of context
It is worth comparing the complication rates of assisted dying procedures with rates for other medical interventions to provide an appropriate context so that they may be realistically interpreted.
For example, a study of common over-the-counter analgesics for short-term pain management2 found that significant adverse effects occurred amongst 13.7% of ibuprofen users, 14.5% of paracetamol useres and 18.7% of aspirin users.
In another example, an anlaysis of primary research about surgical outcomes found that 14.4% had adverse events, almost half of which (47.5%) were moderate to fatal in severity.3
Conclusion
The study is a solid synthesis of research data and indicates that assisted dying is accessed sparingly and in accordance with the intentions of each legislature.
The adverse event rate for assisted dying appears to be substantially lower than the rate of adverse events in the use of common over-the-counter analgesics and in surgery.
References
Emanuel, EJ, Onwuteaka-Philipsen, BD, Urwin, JW & Cohen, J 2016, 'Attitudes and practices of euthanasia and physician-assisted suicide in the united states, canada, and europe', JAMA, 316(1), pp. 79-90.
Moore, N, Ganse, EV, Parc, J-ML, Wall, R, Schneid, H, Farhan, M, Verrière, F & Pelen, F 1999, 'The PAIN Study: Paracetamol, Aspirin and Ibuprofen new tolerability study', Clinical Drug Investigation, 18(2), pp. 89-98.
Anderson, O, Davis, R, Hanna, GB & Vincent, CA 2013, 'Surgical adverse events: a systematic review', Am J Surg, 206(2), pp. 253-62.
Blog by Neil FrancisPosted on Thursday 12th May 2016 at 4:30pm
The more anti-euthanasia campaigner Mr Wesley Smith publishes, the more I think he’s missed his true vocation as a comedian. His latest comical gig against assisted dying is a gem.
Mr Smith starts with the case of two Californian doctors found guilty of Medicare fraud: billing fake hospice care for patients who weren't terminally ill. He artfully turns the story into a series of anti-assisted-dying gags.
Who’s on first, What’s on second?
Mr Smith directly connects the money-grabbing fraud case with the Obama administration, ribbing us that the President and federal authorities won’t hold doctors accountable for breaking assisted suicide law. Mr Smith, an attorney, is holding his breath to see if his audience figures out this little joke: oh, the confused jurisdiction names… right!
The Death With Dignity laws are State laws. If the law is broken it is State responsibility to pursue and prosecute offenders. The Feds have no jurisdiction. If, however, Medicare has been defrauded then it’s a Federal matter (FBI): and the Feds did indeed investigate and prosecute.
It’s a bit like the Laurel and Hardy confused “Who’s on first, What’s on second” name sketch, isn’t it? But only if you get it. Grin.
I say, I say, I say: what’s worse—being evil or being dead?
Mr Smith then refers to the case of Michael Freeland, an Oregonian dying of lung cancer who considered using the Death With Dignity Act. Citing himself and referring to the physician who prescribed lethal medication, Mr Smith compares Dr Peter Reagan with the Medicare fraudsters, saying that Dr Reagan “regularly takes on patients solely for the purpose of facilitating their suicides.”
Defamation is always good for a cackle. It’s so droll, like saying that Mr Smith “opposes assisted dying solely because of the great value of redemptive suffering whether others agree or not.” Which, of course, your dear writer is not saying (because Mr Smith has already stated on the record that he doesn't think suffering is redemptive).I’m just saying, you know, for laughs.
Wesley Smith jokes that Dr Peter Reagan is both evil and dead.
To add even greater mirth, Mr Smith describes Dr Reagan as “now late”. OMG, I've met Dr Reagan and he’s a top fellow. He’s died!? No, he hasn't. Fortunately, like Mark Twain, Dr Reagan happily reports that news of his death has been greatly exaggerated.
Phew, comic relief—what a hoot.
The Clause you have when you’re not having a Clause
Mr Smith then tells the one about how doctors ordinarily have to comply with an accepted medical “standard of care,” but that “death doctors” (love those stereotypes, chuckle!) only have to act in “good faith,” which, Mr Smith razzes us, is quite hard to assess. Oh. Awkward audience silence; a cricket chirps. Um, punchline please?
You have to supply your own punchline for this quip I’m afraid, because Mr Smith rather absent-mindedly forgets to. The Oregon Death With Dignity Act 1997 says explicitly in Clause 126.885 §4.01(7), “No provision [of this Act] shall be construed to allow a lower standard of care…”
Ah, more comic relief: the old 'pull-the-wool-over-your-eyes' caper, chortle.
The flip-flop routine
But the most comical gag is the one I reckon Mr Smith doesn’t even realise he’s told: the joke that we’re all going to die from lethal prescriptions, artfully developed by featuring someone he carefully points out didn’t take the lethal prescription. We just love a good flip-flop. LOL.
Oh, that and teasing us that the Medicare fraud case in which the purpose was to get more money is a great story against assisted dying whose purpose, he banters, is to get less (save) money. Double flip-flop: Ta-ching!
Blog by Neil FrancisPosted on Saturday 2nd January 2016 at 12:35am
Dr William Toffler (left) acknowledges no slippery slope cause-and-effect evidence, with Drs Bentz and Stevens
A new scholarly journal focused on end-of-life ethics, decision-making and practice has just been launched: the Journal of Assisted Dying. In the first article, claims by Oregon lobby group Physicians for Compassionate Care (PCC), including Doctors Bill (William) Toffler and Ken Stevens (and others) are assessed against empirical evidence and found to be completely wrong, or highly misleading as a result of selective use of data.
The new scholarly journal, the Journal of Assisted Dying, is dedicated to careful and holistic analysis of evidence in regard to the various forms of assisted dying that are lawful in a number of jurisdictions around the world... and to practices in jurisdictions where assisted dying remains illegal.
In the first article of a series on Oregon, I examine claims and speculations made by various doctors (and others who quote them), that Oregon has the second-highest suicide rate in the USA (or is always in the top 10), that Oregon's Death With Dignity Act has resulted a massive increase in the state's general suicide rate, and other astonishing statements.
Of course, the empirical evidence from the Oregon Health Authority and from the USA Centers for Disease Control and Prevention does not support these statements and interpretations, and I analyse and critique the evidence.
Some of the claims are just plain factually and hugely wrong. Others are the result of failing to read their sources more carefully, misunderstanding what the data actually represents. Still further claims are made on the basis of selectively-chosen statements from government reports, while omitting statements that are contrary to, or provide alternative and well-researched explanations for Oregon's recently rising general suicide rate.
Drs Toffler and Stevens have even published some of their claims and speculations in the British Medical Journal.1 It goes to show that even good journals sometimes publish bunkum: their article was a letter to the editor rather than peer-reviewed research. Great care is required to sort real evidence from hype and opinion.
Ultimately, Dr Bill Toffler of PCC has acknowledged on video that there is no cause-and-effect evidence between Oregon's Death With Dignity Act and Oregon's suicide rate, an acknowledgement that went unchallenged by his two PCC colleagues present at the time, Dr Ken Stevens and Dr Chuck (Charles) Bentz. You can see Dr Toffler's statement here (at 10'50").
The Journal of Assisted Dying is an open-access journal, and you can read the full article here.
-----
1. Toffler, WL & Stevens, K 2015, 'Re: Assisted dying: law and practice around the world', BMJ, vol. 351, 19 Aug, p. h4481.
Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 1, no. 1, pp. 1–6.
Abstract
Background: Several physicians have speculated that Oregon’s general suicide rate is evidence of suicide contagion as a result of Oregon’s Death With Dignity Act (‘the Act’). Methods: Search and analysis of physician and related online sources of Oregon suicide contagion speculation; retrieval and analysis of cited Centers for Disease Control and Prevention (CDC) and other publications relied upon; analysis of authoritative, public Government mortality data for Oregon and other USA states. Results: Several physicians have speculated about Oregon suicide statistics in a manner that is not supported by the cited publications, or by public CDC mortality database data. The claims variously (a) misrepresent key data in the publications, (b) omit information in the publications that is at variance with suicide contagion speculation, and (c) overlook other significant information at variance with speculation. The physicians have previously acknowledged inability to prove perceived “slippery slope” effects of the Act. Other opponents of the Act have republished the physicians’ erroneous information. Conclusions: Evidence advanced by several physicians to speculate that Oregon’s Death With Dignity Act causes suicide contagion in Oregon is variously false, misleading or highly selective—omitting key facts—and has arisen even though the physicians acknowledge they have no proof of ‘slippery slope’ effects.
Article keywords
suicide contagion, copycat suicide, Werther effect, slippery slope, misinformation, Oregon, Dr William Toffler, Dr Kenneth Stevens, Physicians for Compassionate Care
Full PDF
Download the full PDF: (390Kb)
Citation
Francis, N 2016, 'Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon', Journal of Assisted Dying, vol. 1, no. 1, pp. 1-6.
Blog by Neil FrancisPosted on Wednesday 25th November 2015 at 8:00pm
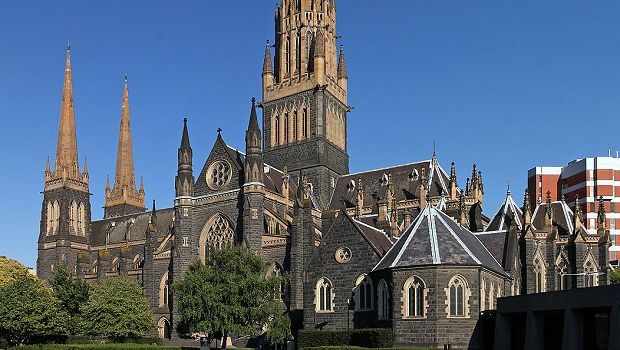
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
On Wednesday 19th November 2015, the Catholic Church appeared before the Victorian Parliament's Legal and Social Issues Committee. Monsignor Anthony Ireland, the Episcopal Vicar for Health, Aged and Disability Care, and Father Anthony Kerin, Episcopal Vicar for Life, Marriage and Family gave evidence about end-of-life decision making. They made a factually wrong allegation about Oregon during their testimony.
Anthony Ireland spoke first, making it clear that they were appearing before the Committee with delegated authority from the Catholic Archbishop of Melbourne (Denis Hart) and with the endorsement of the Victorian Catholic Bishops. He emphasised that "the Catholic Archdiocese of Melbourne does not come to this Committee with fanciful or frivolous arguments."
During question time. Committee Chair Edward O'Donohue asked the Vicars if they had any evidence from lawful jurisdictions to back up their claim that legalising assisted dying would result in a significant reduction in medical research. The Vicars flailed about with vague hypotheticals, but no evidence.
Committee Deputy Chair Nina Springle remarked that some of their testimony was inconsistent with direct evidence from lawful jurisdictions and invited them to reflect on the contradictions. To this, Anthony Kerin stated:
"We know, for example, since Oregon legislated, that the standard suicide rate has increased remarkably and alarmingly. It's not yet the largest rate in the US, but it's getting there, when Oregon had a very, very low suicide rate prior to that."
Let's not mince words: the allegation is comprehensively false. In fact it's three false statements all wrapped up into one.
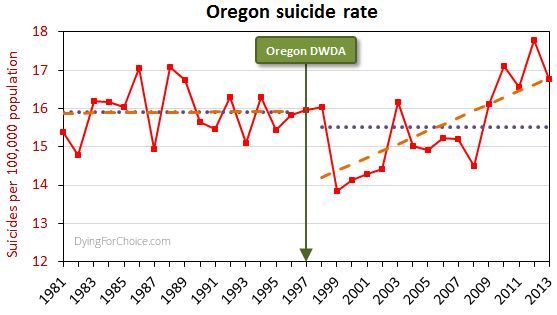
The USA government's CDC mortaility database provides solid empirical data. Here's Oregon's longitudinal suicide rate statistics, including sixteen years before its Death With Dignity Act (DWDA), and sixteen years after.
Here are the pertinent facts about Oregon's general suicide rate:
The average for the 16 years after the DWDA is lower than, but not statistically different from, the 16 years prior to the Act.
There was a massive drop in the suicide rate two years after the DWDA came into effect, and the rate has risen only from there.
The rise from 2000 onwards is repeated in the majority of USA states and in the national average. The trend increase in Oregon is not statistically different from the national trend increase.
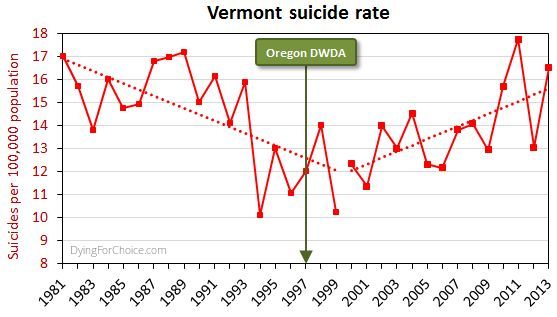
By way of comparison, here's Vermont's suicide rate for the same period.
Now, Vermont didn't have an assisted dying law until 2013, and no assisted deaths occurred under the law in that year, so the suicide rate cannot have been affected by an assisted dying law. Yet the picture is similar to Oregon's.
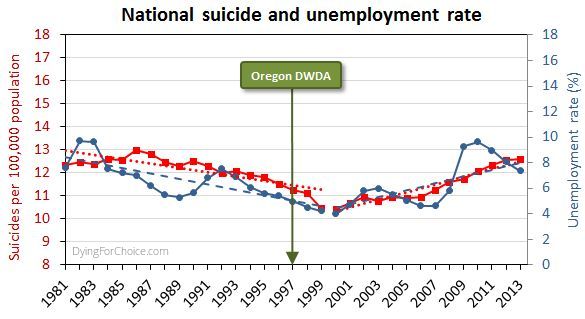
Here's the USA national suicide rate for the same period, with the unemployment rate added.
There are numerous and complex reasons for suicide and for changes in the rate, but a key one in this USA case is unemployment, which after falling in the 1990s rose abruptly from 2000 onwards.
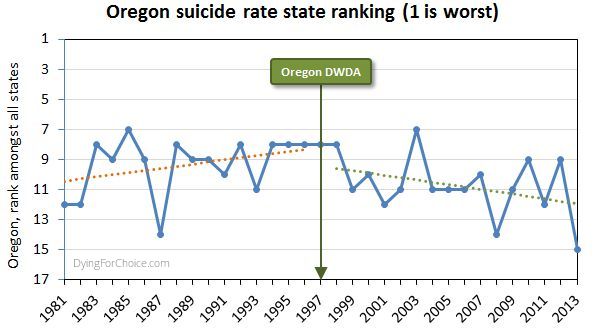
Has Oregon's suicide rate been worsening relative to other USA states, though? The state annual suicide rankings are informative.
Prior to the DWDA, the trend in Oregon's suicide ranking among all USA states was deteriorating (where ranking number one is the highest suicide rate). Since the Act came into effect, the trend is improving. The difference in trends is statistically significant. In the sixteen years since the Act came into effect, Oregon has appeared in the "top ten" six times, compared with twelve times in the 16 years prior to the Act.
So, let's examine the three elements of the Catholic Church's statement:
1. "Since Oregon legislated, the standard suicide rate has increased remarkably and alarmingly"
This statement is false by omission. It is critically relevant to mention that Oregon's suicide rate dropped massively two years after the DWDA came into effect. Only after 2000 did it begin to rise—like most states and nationally—and in response to a rising unemployment rate.
2. "Oregon had a very, very low suicide rate prior to that [the DWDA]"
This statement is completely false. Oregon's mean rate suicide for 16 years after the act is not significantly different from the mean for 16 years prior to the Act. Indeed, government data back to 1968 shows Oregon's general suicide rate has always been high and never "low", let alone "very, very low".
3. It's not yet the largest rate in the US, but it's getting there"
This statement is completely false. Oregon's suicide ranking amongst USA states was worsening prior to the DWDA, but has been improving since.
It's very disappointing indeed that the Catholic Archdiocese of Melbourne would offer such profoundly false testimony to a legislative committee making inquiries on behalf of the people of Victoria. The offense is all the more grevious because of the unequivocal manner in which the statement was made, and that the witnesses specifically stated they did not bring any fanciful or frivolous arguments to the Committee.
It's time to comprehensively stamp out false information about assisted dying, no matter how fervently it might be believed by its proponents. Watch this space: there's plenty more to come!
Blog by Neil FrancisPosted on Thursday 12th November 2015 at 5:35am
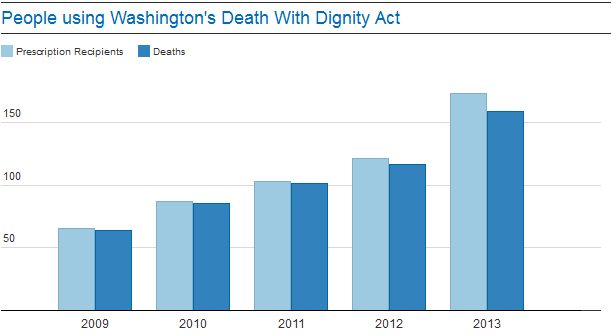
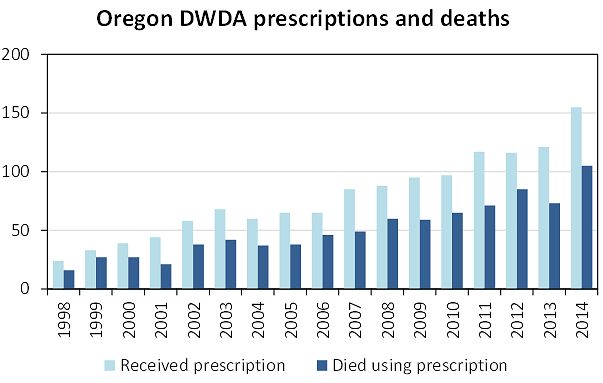
I was browsing the internet the other day checking out commentary on assisted dying in Oregon and Washington state in the USA, and came across an argument in The Guardian—complete with a chart of 'evidence'—that unlike in Oregon, almost all folks who receive a prescription under Washington's Death With Dignity Act (DWDA) die from taking it. 'Eh!?' I thought to myself. I've read all the Washington annual DWDA reports and analysed the data in my own spreadsheets. What The Guardian says is simply not true. How so?
In an editorial on July 18, 2014, The Guardian attempted to estimate the number of people who might use an assisted dying law if it were legalised in the UK. They noted that around a third of Oregonians receiving a prescription under the DWDA died not having taken it. But, they said, "the figures in Washington look quite different. For instance, there isn’t as large a gap in numbers between those who were given prescriptions and those who died." And they offer this chart, which essentially reproduces Figure 2 of Washington's 2013 DWDA annual report, as evidence.
Therein lies a significant problem: the time-poor mistake of grabbing some data out of a report and reproducing it without reading the whole report to understand what the data represents or what it means, and, more particularly, what it doesn't mean.
The thing about the Washington DWDA annual reports, when you read them properly, is that they generally report statistics for all people who have qualified under the Act, i.e. have passed all the critieria and had a prescription written. This is different from the Oregon reports, where most of the statistics relate to people who died by ingenstion of their prescription. This can account for some discrepancies between the two states, and caution in comparing certain statistics.
But the bigger issue, and the cause of the misunderstanding of The Guardian, was twofold. Firstly, as explained, the Washington data quoted was for total deaths of DWDA qualifiers, not of deaths by ingestion of the prescription. Secondly, it is longitudinal data for the deaths of DWDA qualifiers who died in any year, allocated to the year of their first qualification under the DWDA: i.e. backdated.
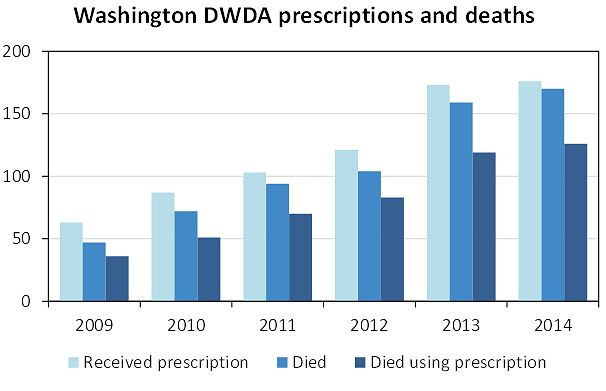
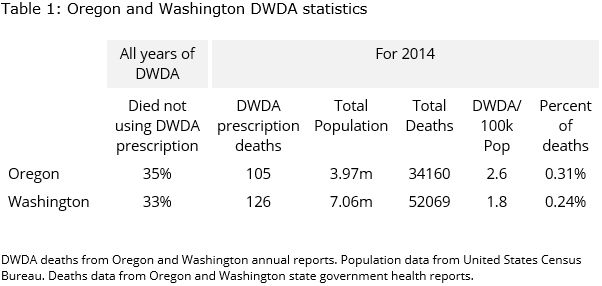
Oregon doesn't report its data in this way, so comparisons cannot be made on that basis. Both states do report the net number of deaths within a calendar year, so that provides a basis for useful comparison. Using this basis, the Washington data looks like this (updated with avialable 2014 data):
The comparable data from Oregon (without 'Died' because that statistic is not reported in a way that can be compared), looks like this:
So, Oregon and Washington are indeed quite similar. Overall statistics are:
Nearly the same proportion of those who die in relation to Washington's DWDA but don't use their medication, as do in Oregon. That's quite a different picture from the one created in understandable haste by The Guardian.
VideoPosted on Thursday 10th September 2015 at 8:20pm
In this thirteen minute video, Oregonians share their experiences of the State's Death With Dignity Act, in effect since 1997. How the Act has worked successfully is described from the medical, palliative care, patient advocate, hospice, legislator and other perspectives, including the daughter of an individual who used the Act.
Part 1 covers attitudes and apprenehsions prior to the Act coming into effect.
Part 2 (2'05") reveals how patient-family-doctor conversations have improved immensely since the Act came into effect.
Part 3 (4'25") discusses the modest numbers of patients using the Act, and that many more Oregonians achieve peace of mind knowing they have a choice even if they don't use it.
Part 4 (7'30") describes how people are free to participate or not, that it is not the 'vulnerable and disenfranchised' who use the Act, and that only minor changes have been made to the Act in order to clarify certain matters, such as residency status.
Part 5 (10"50') concludes with opponents acknowledging there's no evidence for their claim that the Act has caused a 'slippery slope' effect, and State leaders clarifying that the Act has worked as intended, with positive outcomes for the people of Oregon.