An argument that superficially seems intuitively attractive, true or real, but is in fact meaningless or nonsensical.
Netherlands 'suicide contagion' from assisted dying: Theo Boer's smoke and mirrors
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 4, no. 1, pp. 1–11.
Abstract
Background: Concerns had been raised about the scientific quality of a 2017 article by ethicist Theo Boer in which he theorised that lawful voluntary assisted dying (VAD) would potentially ‘dampen’ suicide rates, but drew the opposite conclusion: the suggestion that VAD cases have caused higher suicide rates. Methods: A structured, forensic examination of the article was conducted. Results: Numerous serious shortcomings were found, including (a) profound unfamiliarity with the complexity of suicide; (b) lack of a clear and specific pre-hoc methodology; (c) numerous unsupported speculations; (d) cherry-picked data and casual dismissal of data at odds with the conclusion; (e) a simple correlation interpreted as causation while failing to control for any confounding factors; (f) incoherent, contradictory and misleading statements; and (g) multiple editorial errors. Conclusions: Boer’s article is poorly conceived and carelessly assembled, revealing unfamiliarity with both the subject matter and with scientific principles. The conclusions drawn are not supported by the article’s methodology or data. The article offers mere smoke and mirrors to conclude that VAD may increase suicide rates, at odds with wider evidence.
Francis, N 2019, 'Netherlands "suicide contagion" from assisted dying: Theo Boer's smoke and mirrors', Journal of Assisted Dying, vol. 4, no. 1, pp. 1-11.
Blog by Neil FrancisPosted on Thursday 12th October 2017 at 1:50am
The latest religious right 'think tank' lobby group, the Institute for Civil Society.
I challenge the latest religious right commentators opposing Victoria’s Voluntary Assisted Dying Bill to skip the flip-flopping and engage constructively.
They’re at it again. This time it’s the religious right’s latest ‘think tank’ front group, the impressively-named Institute for Civil Society. Sounds grand, doesn’t it?
But if you look into their lot in life, it’s to protect ‘religious freedoms.’ By that, they mean the right to lawfully discriminate against others of whom they disapprove, while at the same time arguing that they not be discriminated against.
Mark Sneddon and Sharon Rodrick of the ‘Institute’ published an opinion piece in Fairfax Media today.
In it, they slam the Victorian Government’s Voluntary Assisted Dying Bill, which was introduced into the Parliament recently.
They level several criticisms at the Bill to say it's not 'safe'. But they could have advanced any criticism of the Bill to claim, as they do, that “the vulnerable will be at risk” — a logical fallacy as I’ve pointed out before. The "vulnerable will be at risk", by circular definition, if the Bill is printed in black ink (as it is) instead of purple, but they didn't complain about the colour of the ink.
The flip-flop
The point is, they flip-flop because they’re remarkably inconsistent in their position. At the same time as pointing out supposed flaws in the Voluntary Assisted Dying Bill, demanding a much higher standard of proof about a number of things, they completely fail in their opinion piece to even mention — let alone demand the same level of safeguards for — an already-legal and equivalent hypothetical risk for the “vulnerable.”
Equivalent hypothetical risk in operation for nearly 30 years
In Victoria, patients have an inalienable right to refuse any and all medical treatment. No reason need be given, even if the treatment is life-saving. The Medical Treatment Act 1998, currently in force, has several safeguards to protect against coercion or undue influence. In Section 5(1), one doctor and “another person” (who can be anybody) must be satisfied that:
“the patient has clearly expressed or indicated a decision”; and
“the patient’s decision is made voluntarily and without inducement or compulsion”; and
“the patient has been informed” about their condition and “has appeared to understand that information”; and
“the patient is of sound mind and has attained the age of 18 years.”
They’re all the legislated safeguards for the refusal of life-saving medical treatment.
And how many cases of undue influence have been prosecuted in Victoria over the nearly 30 years the Medical Treatment Act 1998 has been in effect? Precisely none. Not one.
So much for Messrs Sneddon and Rodrick’s avaricious relatives lurking at every bedside.
A new, equivalent hypothetical risk
The Medical Treatment Planning and Decisions Act 2016, which will come into force in March next year and which extinguishes the Medical Treatment Act 1998 at that time, also contains several similar safeguards for the refusal of life-saving medical treatment.
In witnessing an Advance Care Directive (Section 17), the two signatories, only one of whom must be a medical doctor, must certify that:
the person “appeared to have decision-making capacity” in relation to the documented decisions; and
the person “appeared to understand the nature and effect of each statement”; and
“the person appeared to freely and voluntarily sign the document”; and
“the person signed the document in the presence of the two witnesses”; and
“the witness is not an appointed medical treatment decision maker for the person.”*
In Section 52 of the Act, a health practitioner is forbidden to administer medical treatment if they are aware the patient has refused it, however (lawfully) refused.
This Act was passed in the term of the current Parliament: that is, by the same State MPs who are now considering the Voluntary Assisted Dying Bill.
There was no great fracas over the sensible safeguards spelled out in the new Medical Treatment Planning and Decisions Act. There was no onslaught of “crisis!” op-ed screeds published in newspapers. There were no countless hours of talking heads tut-tutting and painting doomsday scenarios.
It was passed by the Parliament and accepted by the people as striking the right balance.
No safeguards at all in many cases
And that’s it: the sum-total of safeguards to refuse life-saving medical treatment in Victoria. However, if the patient refuses medical treatment verbally, there are no mandated safeguards at all in either old or new Act, because the statutory safeguards apply only to refusal given in writing.
Yet despite all this, Messrs Sneddon and Rodrick rail against safeguards against coercion and elder abuse only in regard to the Voluntary Assisted Dying Bill, in which the safeguards are of a significantly higher calibre, with, for example, mandatory multiple doctor opinions, documentation trail, multiple requests, no go-ahead until approval by an external authority, notifications of numerous kinds, oversight by a specially-established panel, and so on.
It’s obvious what a flip-flop Messrs Sneddon and Rodrick’s demands are in respect of decisions that will foreseably result in death.
Another embarrassing flip-flop
Messrs Sneddon and Rodrick particularly also complain at length at the supposedly ‘lax’ definition of decision-making capacity in the Voluntary Assisted Dying Bill.
That’s a major and embarrassing flip-flop. Here’s why.
The section of the Voluntary Assisted Dying Bill that stipulates those requirements (Section 4) is the same section number 4 that governs the right to refuse of life-saving medical treatment in the Medical Treatment Planning and Decisions Act 2016. Only a few words have been changed to alter the context from refusal of treatment to consideration of assisted dying. Otherwise, the Sections are identical.
Messrs Sneddon and Rodrick don't point this out in their opinion piece. Indeed, I was unable to find online any evidence that they had published any complaint about the provisions when the Medical TreatmentPlanning and Decisions Act was in debate, nor since. If they have, I’d be happy for them to point it out.
Is it all a strategic ruse, anyhow?
It’s pertinent to ask if the objections are a ruse anyhow, because, as Andrew Denton has rightly pointed out, a key opponent strategy is not to give an outright “no” to assisted dying Bills, but to say only “not this Bill” and create an atmosphere of FUD (fear, uncertainty and doubt) so that it is defeated.
A typical ruse example
By way of example, I’ve published an account of how Victorian MP Daniel Mulino published outrageous misinformation about assisted dying. As a result, we had an extended conversation, during which he acknowledged that he had indeed published misinformation. At the end of the conversation I asked if he could support the Government’s Voluntary Assisted Dying Bill. (He’s a member of said Government.)
No, it’s too liberal, he said, pointing to Oregon’s Death With Dignity Act, now in force for nearly 20 years, as a more conservative approach. So I asked him if he would support a Bill like Oregon’s.
No, he said, there were still concerns about it.
By now you’ve spotted the merely incremental withdrawal of supposed possible support. So I asked him outright if there was any form of assisted dying Bill he could support.
The relevant word within a long discourse: No.
And there’s the answer that belies the political strategy. It doesn’t matter one whit what provisions are included in an assisted dying Bill, just criticize a bunch of provisions and create FUD to defeat it.
A direct challenge to Messrs Sneddon and Rodrick
If “doubters of this Bill” are genuine about permitting assisted dying in some defined circumstances, the duty is on them to define those circumstances and recommend wording to enact it.
And that’s the challenge I throw down directly to Messrs Sneddon and Rodrick. Don’t just bitch and gripe: define precisely what provisions and wording you think would be acceptable.
If you fail to stipulate what you deem acceptable, then your opposition to “this flawed Bill” is, like the supposedly ‘soft’ opposition of other campaigners in the negative, merely a ruse.
And that’s rather suggested by your deliberate use of the term “killing” for what most Australians believe to be an understandable and welcome release. But let’s give you the benefit of the doubt… for now.
Will you rise to the constructive challenge, or lurk in the shadows merely making snide remarks and flip-flopping?
----
* Section 62 of the Act also requires a doctor to notify the Public Advocate if “significant treatment” is refused — but only if it is refused by a substitute decision maker on behalf of the patient: not by the patient herself. And “significant treatment” is defined as treatments (not non-treatments) which are likely to have a serious impact on the patient (bodily intrusion, risk to life, side effects or distress). “Significant treatment” in the Act does not mean treatment whose refusal may result in death.
Blog by Neil FrancisPosted on Tuesday 19th September 2017 at 10:30pm
The Age reports on the three AMA dcotors' appearance at Spring Street
As reported in The Age, on Tuesday this week three AMA doctors fronted the Victorian Parliament to spread the word about their perceived horrors of an assisted dying law. Their arguments don’t hold water and politicians should see them for what they are: utter nonsense.
Doctors Stephen Parnis, Mukesh Haikerwal and Mark Yates say they will continue to lobby politicians.
With what?
Here is the ‘substance’ of their arguments — a sticky blomonge of the same old confected and discredited claims.
The vulnerable will be at risk
Dr Parnis said that such a law “puts the most frail and vulnerable in our community — the dying — at profound risk,” pointing to coercion, and patients not getting the medical care they need.
As I’ve explained before, the claim is flapdoodle — circular nonsense.
It’s a circular argument (a logical fallacy) because “the vulnerable” are by definition those “at risk” and vice versa. While the circularity makes the claim about assisted dying risks seem true, it's a false imputation.
By way of comparison, we could equally say that “the vulnerable will be at risk if we wear yellow socks on Wednesdays,” so we should outlaw that as well. Or anything else of which we disapprove and make our argument seem valid by attaching it to “the vulnerable being at risk.”
Let’s not talk about it
Dr Yates argued that the Parliament should not be pursing “divisive legislation.” That’s also a false argument because it's merely an appeal to emotion: avoiding legislating anything upon which there is any disagreement and discomfort. The consequence of this argument is to not legislate at all.
Patient trust in doctors
They also argued that assisted dying legislation would “change the doctor-patient relationship” — by which they mean “damage the relationship,” or they wouldn’t have mentioned it.
Again, as I have shown before, the empirical evidence from around the world is consistent with improved, not damaged, patient trust in doctors where assisted dying is legal.
The massive AMA flip-flop
But, as I’ve also pointed out before, the real telltale of the AMA doctors’ farcical representation to the Victorian Parliament is this: while opposing assisted dying legislation because patients might be pressured, subtly or otherwise, to choose death, the AMA officially endorses the right to refuse medical treatment, which includes life-saving treatment.
The hypothetical risk of patients being encouraged to refuse life-saving medical treatment is identical in kind to that of assisted dying. Yet in Victoria, the right to refuse is protected by just three statutory safeguards, while the assisted dying legislation is founded on no fewer than 68 safeguards.
So the AMA incoherently promotes one hypothetical pressure-to-die pathway with only three protections, while cruelly opposing a parallel path with an armada of protections. Let's award 10 out of 10 for the impressive flip-flop manoeuvre.
Conclusion
The AMA doctors’ claims are without merit and advancing them does no favours to their professional credibility.
Blog by Neil FrancisPosted on Sunday 6th August 2017 at 3:36am
Victorian MP Daniel Mulino's minority report contains multiple serious errors and misinformation.
Last year, the Victorian Parliament's Legal and Social Issues Committee concluded an extensive investigation into end of life choices, publishing a report of over 400 pages recommending improvements to palliative care and for assisted dying. Catholic-backed Shop, Distributive and Allied Employees' Association (‘shoppies’ union) Labor member of the Victorian Parliament Mr Daniel Mulino furnished his own minority report, opposing the majority recommendation for assisted dying law reform. That’s entirely his right. However, his report contains multiple, serious cases of misinformation. He must withdraw his report.
Daniel Mulino, Labor parliamentary member for the Victorian Region of Eastern Victoria,1 and a member of the Catholic-backed ‘shoppies’ union,2 was a member of the Legal and Social Issues Committee that thoroughly investigated end of life decision making and produced a 400+ page report in 2016 making recommendations for law reform and regulation.
Mr Mulino furnished a “minority report” as an addendum to the main report in order to oppose the Committee’s recommendation that assisted dying be legalised.3
Promoted by Catholics to Catholics
Mr Paul Russell, South Australian publisher of the Catholic anti-euthanasia website ‘HOPE,’§ says this of Mr Mulino’s minority report in the Catholic lawyer association’s blog:4
“Daniel Mulino MLC's analysis should be read first, before the Majority Report. It forms not only a sound academic and rigorous approach but also, by implication, is damning of the narrow, outcome focus of the Majority Report.”
How sweet of Mr Russell to so generously plug Mr Mulino’s report. But, in gushing about the ‘sound academic and rigorous approach’ he claims to be in it, shows that he doesn't understand what constitutes proper and sound evidence, and that he's easily impressed by charts and lots of ‘literature’ citations.
Numerous fundamental faults
The reality is very different.
Rather than bore you with a mind-numbing blow-by-blow dissertation on the numerous fundamental faults in Mr Mulino’s report, I’ll demonstrate how the report cherry-picks, misquotes and misunderstands its way through the evidence, via four revealing examples.
Example 1. Cherry-picking ‘helpful’ data
Mr Mulino’s minority report illustrates the rise in number of assisted deaths in the Netherlands and Belgium, and produces some statistics (Figures 1 & 2 are directly from his minority report).
Figures 1 and 2 (of Mr Mulino’s minority report): Assisted deaths in Belgium and the Netherlands
Note that Belgian data is for the years 2003–15, but the Netherlands only for the years 2008–15. That’s odd, because the euthanasia Acts for both countries came into effect in 2002, and so 2003 was the first full year for both.
Mr Mulino doesn’t point out that his report treats the two countries differentially, and provides no explanation as to why. We might notice, however, that the dicrepancy has the consequence of making his claims look 'better.'
Using Mr Mulino’s presentation style, Figure 3 illustrates all the relevant data for the Netherlands.
Figure 3: The full Netherlands data Source: Official Euthanasia Commission reports
As you can see, there is a virtual flatline between 2003 and 2007. Indeed, there is even a tiny drop in numbers between 2005–06. This is an inconvenient truth to Mr Mulino’s thesis that there has been a consistent massive rise in numbers. It also substantially reduces the compound annual growth rate he wrongly quotes for just 2008–15.
He’s also cherry-picked only raw data. In fact, the only valid way to compare year to year, and jurisdiction to jurisdiction, is to use the rate for each year: that is, the number of assisted deaths as a proportion of total deaths in the same year and jurisdiction, so that you’re comparing apples with apples. It's necessary because the total deaths count goes down and (mostly) up a bit each year. The official government statistics for total deaths by year for both countries are readily available online, so there’s no excuse for not using them.
When you calculate the rates, you get validly-comparable results, as I illustrate in Figure 4.
Figure 4: Rate of assisted dying as a percent off all deaths in the Netherlands and Belgium 2003–2015 Sources: Official government statistics; Euthanasia Commission reports
As I explain in my detailed research whitepaper on Benelux assisted dying,5 these are sigmoid (stretched-S) shaped curves which are typical of human behaviour change. And there is a drop in the rate in both countries in 2015, which Mr Mulino doesn’t report.
My Benelux whitepaper also reports the data from Luxembourg (Figure 5), which Mr Mulino fails to mention, even though it has legislation, since 2009, almost identical to the Netherlands and Belgium, and the Luxembourg government's data is freely available online.
Figure 5: Rate of assisted dying in the three lawful Benelux countries Sources: Official government statistics; Euthanasia Commission reports
Luxembourg’s data (yellow in Figure 5; no data available yet for 2015), is also an inconvenient truth to the case Mr Mulino attempts to prosecute. There’s no substantial rise.
Example 2. Comparing apples with oranges: mis-matching data
Mr Mulino again fails to compare apples with apples. Take, for example, his vocal claim that the annual total death counts for the Netherlands decreased at the same time as the total counts for assisted dying increased.
When you look at the data he’s used (the citation for the negative total deaths trend he quotes in his Table 2), you find that he’s used total death data for 2000–10, which is falling, while his assisted dying data is for 2008–15, which is rising.
This just isn’t on: it’s completely invalid to compare data like this from one period with data from another period to claim or imply a causal relationship. Of what possible relevance is the total death data for 2000–02, while his total deaths data for 2011–15 is missing? I illustrate the full story in Figure 6.
Figure 6: Netherlands total and assisted deaths for different periods Sources: Official government statistics; Euthanasia Commission reports
The solid blue and orange lines are data Mr Mulino used and reported, and their dotted ends are data that he omitted. It’s easy to see that the total deaths data his report inappropriately relies upon has a negative (downwards) slope (left-hand blue dashes), while the matching total deaths data he should have used has a positive (upwards) slope (right-hand blue dashes). Valid comparison gives lie to his claim.
Example 3. White is the new black: Misquoting the opposite
Mr Mulino’s report also argues that there’s ample evidence that a significant proportion of people with depression are gaining access to assisted dying:
“Ganzini et al, in a broad ranging review of instances of assisted dying in Oregon, found that twenty percent of the patients had symptoms of depression.” [Italics mine]
This assertion is nonchalantly plucked from the review6 without reading it properly, seemingly to support his thesis. In fact, the source does the exact opposite. Figure 7 is an image of the Abstract, where it says in large print, right up front:
“Twenty percent of the patients had symptoms of depression; none of these patients received a prescription for a lethal medication.” [Emphasis is mine]
Figure 7: The paper Abstract articulates exactly the opposite of Mr Mulino’s claim Source: Ganzini et al 20006
Had Mr Mulino bothered to read either the abstract or the methodology of this study properly, he would have realised that the doctor sample was of those eligible to prescribe under Oregon’s Death With Dignity Act, not just those who had, and that none of the study's patients who were assessed with possible depression had accessed an assisted death.
It's not like the information was hard to find — his report cites literally half a sentence to support his claim, when the full sentence says the opposite.
Example 4. Any port in a storm: Cherry-picking, misunderstanding and misrepresenting out-of-date data
In attempting to establish a 'slippery slope' from voluntary, to non-voluntary euthanasia (NVE) — a practice where doctors may hasten death (e.g. by administering increasing doses of opioids) when the patient hasn’t explicitly requested it — Mr Mulino states in his minority report:
“Two countries with the highest rates of this type of end-of-life (Belgium at 1.5% and the Netherlands at 0.60%) allowed the practice of euthanasia and assisted dying.”
Oh dear, Mr Mulino's report cherry-picks again. Just look at his source.7 The study, published in 2003, contains Table 2, with the relevant data in it (Figure 8).
Figure 8: Table 2 from the 2003 study Mr Mulino cites Source: van der Heide et al 20037
There are no fewer than five major offences Mr Mulino commits here.
Firstly, look at the table. I’ve highlighted the line in yellow from which Mr Mulino draws his figures of 1.5% for Belgium and 0.60% for the Netherlands. You can immediately and easily see that Denmark’s rate of 0.67% is higher than the Netherlands' of 0.60%.
So, Mr Mulino’s statement mentioning only Belgium and the Netherlands with “highest NVE rates” is misleading. He failed to either report or explain why Denmark’s rate is higher than the Netherlands, while Denmark doesn’t have an assisted dying law; the opposite of his thesis.
Secondly, he also fails to mention Switzerland’s NVE rate of 0.42%, or to explain that it’s lower than the Netherlands and Belgium. That’s highly relevant, because Switzerland has the world’s oldest assisted dying law — in effect since 1942 — and its statute contains none of the safeguards in the Belgian and Dutch Acts. This too is at odds with Mr Mulino’s thesis.
Thirdly, if Mr Mulino had read the study properly instead of just cherry-picking convenient figures from it, he would have noticed in the methodology section that the fieldwork (doctors filling in questionnaires) was completed in 2001 and early 2002, that is, before either the Netherlands or Belgian Acts came into effect later in 2002 (the Netherlands in April and Belgium in September).
Thus, the Dutch and Belgian data points Mr Mulino advances as ‘evidence’ of an NVE ‘slippery slope’ from legislated assisted dying have nothing whatever to do with assisted deaths under their Euthanasia Acts, because neither Act existed at the time the study was conducted.
Fourthly, he is resorting here to a single point-in-time study, which has little to no scientific power to establish ‘causation’. To really establish causation, as a minimum you have to assess longitudinal data, which I show in Figure 9. It demonstrates the precise opposite of Mr Mulino's ‘slippery slope’ thesis that voluntary euthanasia causes NVE, which if true would lead to a significant increase in the NVE rate in both countries after statutory legalisation.
Figure 9: Longitudinal NVE rates in the Netherlands, Belgium and the UK Sources: Netherlands8; Belgium9; UK10
Both the Dutch and Belgian NVE rates have dropped with high statistical significance since their euthanasia Acts came into effect. Indeed, the NVE rate in the Netherlands is now similar to the rate in the UK, which is acknowledged as the world’s gold standard in palliative care and which hasnever had an assisted dying law. This is consistent with assisted dying law reform shining a bright light on all end of life practices.
It’s not like he simply didn’t know
Fifthly, it’s particularly disappointing that Mr Mulino’s report only cherry-picked outdated data in an attempt to ‘prove’ his case when I had already directly furnished the current relevant evidence to his Committee as a properly-researched formal submission: Figure 9 above is Figure 19 in my submission, and I provided the peer-reviewed research citations for the data.11
Not only that, but the official transcript of my appearance as an expert witness before the parliamentary Committee confirms that Mr Mulino specifically quizzed me on that Figure 19 and I pointed out the sources of its data:12
“Mr MULINO — Figure 19, for example.
Mr FRANCIS — The reference should be in the text. The last sentence on the previous page gives you the citations for that data.
Mr MULINO — Okay.”
Even further, when fellow-Committee-member and Catholic assisted dying opponent Mrs Inga Peulich asked about the same thing (with Mr Mulino present) — “1,000 of those who have been accidentally euthanased in the Netherlands” — I literally put the chart up on the projection screen and explained it in full to the Committee until they had no more questions. The “1000” figure is the approximate rate prior to the Dutch Euthanasia Act, while the rate has dropped significantly since.
The evidence is irrefutable: it’s not like Mr Mulino was merely blissfully unaware of the relevant data contradicting his NVE ‘slippery slope’ claim. His minority report expressly overlooks this robust evidence and instead refers inapproriately to selective and outdated data that seemed to, but didn’t, support his argument.
Five major offences in a single citation: surely Mr Mulino’s report — far from ‘academic and rigorous’ — sets a new record?
A common religious thread?
The NVE ‘slippery slope’ claim is also popular amongst and spread by the Catholic Archdioceses of Melbourne,13 Sydney14 and Brisbane,15 as well as by other Catholic anti-assisted dying lobbyists such as Alex Schadenberg,16 Paul Russell,17 and Professor of Ethics at the Catholic University of Notre Dame Australia, Margaret Somerville.18
Indeed, Mr Mulino’s minority report appears amongst 11 Catholic responses against assisted dying law reform published by the Catholic Archdiocese of Melbourne (Figure 10).
Figure 10: Daniel Mulino’s minority report appears amongst Catholic responses on the Catholic Archdiocese of Melbourne’s website19
Indeed, Mr Mulino’s linked document doesn’t seem to emanate from his parliamentary office or from wider parliamentary services: the PDF file's metadata reveals that it was authored, electronically at least, by “mmacdonald”.
Calls to both Mr Mulino's electorate office and to the Parliament of Victoria confirm there is no "M Macdonald" at either. I did, however, find online one Matthew Macdonald, researcher and Executive Officer of the Catholic Archdiocese of Melbourne’s (CAM) Office for Life, Marriage and Family — in other words, the same organisation that published the list in Figure 10 containing the link to Mr Mulino’s minority report.
Mr Macdonald is also listed as the CAM's official contact person in its submission (#705) opposing assisted dying to the Victorian Parliament's inquiry into end of life choices.20 Both the CAM and Mulino reports also refer to a journal paper by Catholic doctor José Pereira,21 and neither report mentions the subsequent evidential rebuttal outlining why Pereira's claims were merely "smoke and mirrors".22 Even more curiously, the Pereira paper is included in Mr Merlino's minority report bibliography, though his report doesn't actually cite it as the CAM submission does.
The CAM parliamentary submission was authorised and signed by Episcopal Vicars Anthony Ireland and Anthony Kerin, who also appeared as witnesses before the parliamentary Committee, during which they told, as I've explained, a whopping great falsehood about Oregon.23
Conclusion
Contrary to Paul Russell’s enthusiastic claim that Daniel Mulino’s minority report provides a ‘rigorous’ case against assisted dying law reform, the report merely serves as further evidence of how those implacably opposed to assisted dying can cherry-pick, misunderstand and rather desperately clutch their way through their ‘evidence.’
Mr Russell is not an academic expert and one can understand his limited capacity to judge whether work is ‘scholarly.’ However, Mr Mulino holds a PhD in economics from Yale,* so it’s quite astonishing that he published a ‘researched’ report containing multiple major flaws, including outdated and cherry-picked data contrary to more recent, direct and relevant evidence of which he was specifically aware, actively inquired into and had explained and cited to him in full.
These anomolies beg the question: did Matthew McDonald or someone else at the Catholic Archdiocese of Melbourne write Mr Mulino’s report for him? Mr Mulino needs to explain himself, since regardless of who authoried it, he signed it off in his own name and is therefore ultimately responsible for it.
Given the multiple fundamental errors, the honourable course for Mr Mulino to pursue is to withdraw his minority report.
The question is: will he rise to the occasion?
Addendum: A missed opportunity for primary research
Mr Mulino — as well as Mrs Peulich who also wrote a minority report against assisted dying — declined to join other members of the parliamentary Committee on an official overseas fact-finding tour to jurisdictions where assisted dying is lawful. This was a critical opportunity for Committee members to directly quiz proponents, opponents, researchers, regulators, legislators and others with direct experience. It would have given them invaluable opportunities to directly examine and test assumptions, hypotheses and performance. How curious then that these two non-participataing Committee members each furnished a minority report opposing the majority recommendation to legalise assisted dying in Victoria.
---------------
§ The HOPE website is an initiative of the Australian Family Association (AFA), a faith-based organisation founded by Australia’s most famous Catholic, B. A. Santamaria. Mr Russell is a former Vice President of the AFA, and a former Senior Officer for Family and Life at the Catholic Archdiocese of Adelaide.
* While Mr Mulino holds a PhD and would be entitled to be addressed as “Dr”, his Parliamentary title is “Mr”.
Ganzini, L, Nelson, HD, Schmidt, TA, Kraemer, DF, Delorit, MA & Lee, MA 2000, 'Physicians' experiences with the Oregon Death with Dignity Act', New England Journal of Medicine, 342(8), pp. 557-563.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, 362(9381), pp. 345-350.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, 380(9845), pp. 908-915.
Bilsen, J, Cohen, J, Chambaere, K, Pousset, G, Onwuteaka-Philipsen, BD, Mortier, F & Deliens, L 2009, 'Medical end-of-life practices under the euthanasia law in Belgium', New England Journal of Medicine, 361(11), pp. 1119-1121.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, 23(3), pp. 198-204.
Francis, N 2015, Submission to the Parliament of Victoria Standing Committee on Legal and Social Issues on the Inquiry into End of Life Choices, DyingForChoice.com, Melbourne, pp. 51.
Parliament of Victoria 2015, Standing Committee on Legal and Social Issues inquiry into end-of-life choices: Witness-Mr Neil Francis, DyingForChoice.com, Melbourne, pp. 10.
Schadenberg, A 2013, Exposing vulnerable people to euthanasia and assisted suicide, Ross Lattner, London ON.
Russell, P 2015, Submission 926: Submission to the Victorian Legal and Social Issues Committee inquiry into end of life choices, HOPE, Melbourne, pp. 56.
Catholic Archdiocese of Melbourne 2015, Submission to the Legal & Social Issues Committee: Inquiry into end of life choices, Submission 705, Melbourne, pp. 16.
Pereira, J 2011, 'Legalizing euthanasia or assisted suicide: the illusion of safeguards and controls', Current Oncology, vol. 18, no. 2, pp. e38-48.
Downie, J, Chambaere, K & Bernheim, JL 2012, 'Pereira's attack on legalizing euthanasia or assisted suicide: smoke and mirrors', Current Oncology, vol. 19, no. 3, Jun, pp. 133-8.
The F filesPosted on Friday 14th October 2016 at 1:21am
BMA House in Tavistock Square, London, home to the British Medical Association since 1925.
The British Medical Association (BMA), in the latest incarnation of its policy on assisted dying (AD), insists that AD must not be legalised in the UK. I argue that its indefensible stance reveals ignorance, incoherence and hubris. It fails to respect the true range of views amongst UK doctors. I expose the comprehensive rot.
The BMA categorically states in its July 2016 policy update on assisted dying:
“The BMA policy … insists that voluntary euthanasia [and] physician-assisted suicide should not be made legal in the UK.” — British Medical Association1
BMA comprehensively out of touch
The BMA claims to represent UK doctors—though fewer than half are members. What is the empirical evidence for UK doctor attitudes toward assisted dying?
In a 2009 survey,2 35% said that AD should definitely or probably be legalised. The same study also found that 35% of UK doctors said AD should definitely not be lawful even in cases of terminal illness. That is, the stance of just 35% of UK doctors was identical to the BMA’s—insisting that it not be lawful, while an equal proportion thought AD could be legalised. “Greater religiosity” was the strongest correlative factor with opposition to lawful AD.
Indeed, numerous studies have found a substantial minority of UK doctors in favour of lawful AD, including results approaching equality with opponents.3 Even a survey commissioned by the UK Catholic Medical Association in 2003 found around 25% of UK doctors in favour of AD and who would practice it if legalised.4
UK doctor support for AD, then, is substantial and hardly restricted to a mere handful of fringe-dwelling medical crackpots.
Ignorant and disrespectful BMA stance
It is untenable that the BMA unilaterally ‘respects’ the views of 35% of UK doctors at the same time as expressly disrespecting the views of another significant cohort. Perhaps as in general politics, its power base is more heavily populated with religious souls: those who have a deeper interest in shaping what options others do and don’t have?
Appalling and trivialised ‘rationale’
Let’s take a look at the five moribund reasons the BMA offers in defense of its institutional opposition to AD and see how they use flapdoodle, fudge, fiction, fear-mongering, flip-flop and hubris to ‘advance’ their position.
“Current BMA policy firmly opposes assisted dying for the following [five] key reasons:”
1. Permitting assisted dying for some could put vulnerable people at risk of harm.
Flapdoodle. Firstly, as I have explained before, the “vulnerable at risk” argument is a rhetorical sham. People ‘at risk’ are by definition ‘vulnerable,’ and would still be so if we wore yellow socks on Wednesdays or outlawed pizza. It has nothing to do with AD being legalised or not.
Fudge. Secondly, the BMA ignores repeated reviews published in the professional literature indicating that supposed harms have not eventuated in jurisdictions with lawful assisted dying. Indeed, the quality of medical practice has improved.
Flip-flop. And thirdly, if ‘risk of harm’ was a sufficient condition to deny patients a particular option, we must equally ban the right to refuse life-saving medical treatment (no matter how unwanted or burdensome) because greedy relatives eyeing off the estate might convince the dying patient to refuse. It’s incoherent to oppose assisted dying, but to support refusal of treatment (as the BMA does), in the face of this identical possibility.
2. Such a change would be contrary to the ethics of clinical practice, as the principal purpose of medicine is to improve patients’ quality of life, not to foreshorten it.
Fudge. Medicine has a number of primary purposes. Relief of suffering is one.5 That may come into conflict with another purpose, “the avoidance of premature death and the pursuit of a peaceful death” (which itself has internal conflicts). A dying individual may herself believe that an AD would not be premature, and whose peaceful nature is vastly preferable to continued intolerable and unrelievable suffering.
3. Legalising assisted dying could weaken society's prohibition on killing and undermine the safeguards against non-voluntary euthanasia. Society could embark on a 'slippery slope' with undesirable consequences.
Fear-mongering. Non-voluntary euthanasia (NVE) is currently illegal. It remains illegal even when AD is legalised. The BMA therefore incoherently conjectures that NVE doesn’t occur while it’s illegal (before AD legalisation), but might occur while it is still illegal (after AD legalisation).
Fiction. There are no current ‘safeguards’ against NVE as the BMA statement implies. It is practiced in secret. There are no statutory requirements or reporting standards as there are for AD (where legal). Research clearly demonstrates that NVE occurs everywhere, including the UK. Further, the rate of NVE has significantly decreased in the Netherlands and Belgium since their AD statutes came into effect.
4. For most patients, effective and high quality palliative care can effectively alleviate distressing symptoms associated with the dying process and allay patients' fears.
Flapdoodle. The BMA says “effective … palliative care can effectively alleviate…”: another circular, self-‘proving’ argument.
Hubris. The BMA acknowledges here—as unarguably established in the professional literature—that palliative care can’t help everyone. And that’s precisely what assisted dying law reform is about: for people that palliative care can’t help. But the BMA brushes them under the carpet.
5. Only a minority of people want to end their lives. The rules for the majority should not be changed to accommodate a small group.
Flip-flop. In ‘reasons’ 1 and 3 above, the BMA speculates that too many people will die if AD is legalised. Here is it arguing that too few will. Which is it? Too many or too few? The argument also ignores the international evidence that dying individuals (and their loved ones) experience profound relief merely from knowing that AD is available, even if they don’t pursue it. That itself is good palliative care.
Hubris. And if “not changing the majority's rules to accommodate a small group” were a gold standard as the BMA argues, then there would be no leglisation to (a) ensure facilities access to people with a disability, (b) outlaw discrimination on the basis of race or religion, or (c) allow same-sex marriage: all enshrined in law in the UK.
Hubris argues for ignoring the BMA itself
If, as the BMA argues, we should override the wishes of a group on the basis of its small size, it’s pertinent to consider the size of the UK doctor population: around 0.4% of the total. By comparison, in jurisdictions where AD is legal, around 0.3% (Oregon) to 3.8% (Netherlands) ultimately choose an assisted death.
If we are to ignore 0.3%–3.8% of the population because it’s ‘too small,’ we must equally ignore 0.4% of it. This, by the BMA’s own argument, would be reason to force it to support AD because that’s what the majority (UK population) favour. After all, “the rules for the majority should not be changed to accommodate a small group [of doctors].”
Of course most of us recognise, unlike the BMA, that this is not a ‘popularity contest.’ A stance of neutrality would demonstrate respect for deeply-held views across the spectrum.
Conclusion
The British Medical Association demonstrates profound ignorance about the available evidence, and about UK doctor attitudes. It resorts to fear-mongering speculation, fudge, fiction, flapdoodle, flip-flop and hubris to maintain its indefensible opposition to assisted dying.
The BMA’s stance does a great disservice to the British people. It’s an embarrassment to professional doctors regardless of their stance on assisted dying. The policy deserves to be entirely scrapped, and one of neutrality adopted in its place.
Seale, C 2009, 'Legalisation of euthanasia or physician-assisted suicide: survey of doctors' attitudes', Palliative Medicine, 23(3), Apr, pp. 205-212.
McCormack, R, Clifford, M & Conroy, M 2011, 'Attitudes of UK doctors towards euthanasia and physician-assisted suicide: a systematic literature review', Palliative Medicine, 26(1), pp. 23-33.
Catholic Medical Quarterly 2003, 'Euthanasia and assisted suicide: Results of survey of doctors attitudes', Catholic Medical Quarterly, May, pp. 1-3.
Hastings Center Report 1996, 'The goals of medicine. Setting new priorities', The Hastings Center Report, 26(6), pp. S1-27.
Blog by Neil FrancisPosted on Sunday 28th August 2016 at 12:58am
Brad Mattes' blog containing misleading and evidentially false statements.
The latest misinformation employed by assisted dying opponents is to imply that Belgium’s general suicide rate is high as a consequence of its assisted dying law: i.e. to argue the discredited 'suicide contagion' line which has in the past been peddled about the USA state of Oregon. I have demonstrated that it was false in Oregon, and I equally demonstrate here that it's false in Belgium.
Mr Brad Mattes recently published emotional anti-assisted-dying nonsense in LifeSiteNews. (LifeSiteNews is a Canadian blog site that was established by the conservative Christian Campaign for Life Coalition and which has a primary principle of promoting “traditional Judeo-Christian principles”. Mr Mattes is radio host for Ohio’s Life Issues Institute, an anti-abortion lobby group established by conservative American John C. Willke who claimed that women’s bodies were resistant to pregnancy as a result of rape.)
Putting on the misinformation running shoes
In his blog Mr Mattes quickly establishes a practice of communicating misinformation by first claiming that assisted dying laws have “devastating effects” around the world including Japan and Albania—which don’t have such laws.
He then sprints onwards to the ‘650 babies euthanized in the Netherlands’ claim—which I have already comprehensively exposed as fake in the Journal of Assisted Dying—and then onto the bogus claim that the Netherlands has descended into a mire of ‘killing’ without the patient’s ‘consent,’ contrary to empirical evidence I've published that such actions occur around the world regardless of assisted dying laws, and which have decreased significantly in the Netherlands and Belgium since their assisted dying statutes came into effect in 2002.
Let’s add fries to that
Having served up a lot of fat and salt that might appeal to those on a fast-food anti-assisted-dying diet, he then offers the unqualified statement:
“By the way, Belgium has the second-highest suicide rate (nonrelated to euthanasia) in Western Europe.” — Brad Mattes
The ‘informational’ consequence is unequivocal: by Mr Mattes failing to contextualise this ‘incidental factoid’ in any way, the reader is destined to deduce that it is Belgium’s euthanasia law that causes Belgium’s suicide rate to be the second-highest in Western Europe. In other words, Mr Mattes is another poorly-informed commentator using the 'suicide contagion' line.
But what are the facts?
Depending on the source and year of data, one can certainly argue that Belgium’s general suicide rate is the second-highest in Western Europe. Setting aside for now the serious question of why it is valid to exclude all of the world’s other countries from the comparison, WorldLifeExpectancy.com reports figures that were published in 2014 (Table 1).
Table 1
Country
Suicides*
Finland
15.11
Belgium
14.64
Iceland
14.06
France
12.84
Austria
11.87
Sweden
11.43
Ireland
11.06
Germany
9.59
Switzerland
9.56
Norway
9.28
Denmark
9.19
Luxembourg
9.14
Netherlands
8.54
Portugal
8.49
Turkey
7.92
UK
6.28
Malta
5.75
Spain
5.23
Italy
4.76
Greece
3.86
* Suicides per 100k population, age-adjusted
The table includes all the countries in the wider definition of “Western Europe”, bar four: no suicide statistics are published for Liechtenstein, Monaco, Andorra or San Marino.
As you can see, Belgium is indeed the second-highest. But this begs the question:
If the reason Belgium is the second-highest is due to its assisted dying law, how come Finland, which Mr Mattes doesn't mention by name and which has no such law, is higher?
It also begs the question:
If assisted dying law were the fundamental cause of a high general suicide rate, how come Switzerland (statute since 1942), Luxembourg (statute since 2009) and the Netherlands (practice since the early 1980s and statute since 2002) have rates that are muchlower, all key facts that Mr Mattes also fails to mention?
These are of course indications that the factoid has been included as a cherry-picked morsel of 'proof' because it sounds so compelling as a throw-away sentence amongst the other (false) statements.
But wait, there’s more
We can go further than merely wondering about the country comparisons, by comparing Belgium’s general suicide rate before and after assisted dying law reform. A critical step in establishing causation is to first establish correlation. If there is no correlation, there can be no causation.
Published OECD data shows that in 2013 (the most recent available data), Belgium’s general suicide rate was 16.7 per 100,000 population. What was it before their 2002 law reform? Well in 2000 it was 20.5, in 1990 it was 19.2, … you get the idea.
Has Belgium’s general suicide rate soared (or even increased modestly) since their 2002 assisted dying law came into effect? No. It’s dropped. Indeed, the slight downward trend apparent before the statute came into effect in 2002 has accelerated downward since (Figure 1).
Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Even the headline is misleading
Mr Mattes fails to point out in his blog that assisted dying statutes in Benelux countries (Belgium, the Netherlands and Luxembourg) never restricted access to only the 'terminally ill,' that is, those imminently dying. He also fails to point out that USA states whose laws do restrict assisted dying to the terminally ill—most notably Oregon and Washington—have not changed their statutes in this regard since they came into effect.
Therefore, his headling implying that lawful jurisdictions have broadened their laws from 'only the terminally ill' is also wrong.
Conclusion
Mr Mattes makes multiple false and misleading claims and it’s easy to see his opinion for what it is: an emotional dump that fails to engage with and indeed flies in the face of actual evidence. The latest 'suicide contagion' implication, that assisted dying law causes Belgium’s general suicide rate to be the “second-highest in Western Europe” is evidentially false.
I call on LifeSiteNews to withdraw Mr Mattes' article because it breaches their primary principle:
“1. Accuracy in content is given high priority. News and information tips from readers are encouraged and validated. Valid corrections are always welcome. Writing and research is of a professional calibre.” — LifeSiteNews
Summary of facts
Belgium's general suicide rate is one of the higher ones in Western Europe. However:
At least one country without an assisted dying law has a higher suicide rate, inconsistent with 'suicide contagion' theory.
Other Western Europe countries with assisted dying laws have suicide rates much lower than Belgium's, also at odds with 'suicide contagion' theory.
But the clincher is that the suicide rate in Belgium has dropped, not risen, since their 2002 assisted dying law came into effect.
Blog by Neil FrancisPosted on Sunday 26th June 2016 at 2:05am
Schadenberg and Russell falsely call the Oregon Medical Association the "assisted suicide lobby" in contradiction of the facts.
Last week, Alex Schadenberg wrote—and Paul Russell republished—another nonsense article, this time about medical associations going neutral on assisted dying. They opine that there is no such thing as neutrality. And start out by getting their facts wrong... again.
Got the facts wrong yet again, lads
Messers Schadenberg and Russell claim that the Oregon Medical association is an "assisted suicide lobby" group. Had they bothered to check the rudimentary facts before sounding off, they would have known that the Oregon Medical Association remains neutral toward assisted dying. It reconfirmed its neutral stance as recently as early this month. It does not hold a 'supportive' stance.
How did Schadenberg and Russell come to their conclusion?
American Medical Association AGM
They refer to a motion that the Oregon Medical Association put to the recent annual general meeting of the American Medical Association. The motion sought to establish a process by which the American Medical Association would consult in order to re-evaluate its opposed stance to assisted dying, given that assisted dying is legal in a number of USA States and there are already many doctors who in good conscience provide assistance to die to qualifying patients.
Heavy-handed partisanship
In their usual style of heavy-handed partisanship, Schadenberg and Russell describe the Oregon motion as the "assisted suicide lobby" applying "pressure" to the American Medical Association.
They fail to level the same criticism at another group, the Louisiana Medical Society who put another motion to the meeting. The Louisiana motion sought to expressly confirm and entrench the American Medical Association's currently opposed stance. Schadenberg and Russell fail to criticize the Louisiana motion as "pressure," despite the fact that Oregon's motion was for open consultation, while Louisiana's was for a closed position.
Good sense prevails
In fact, they don't mention the Louisiana motion at all. Why? Because wiser heads prevailed at the national conference. The Louisiana motion was defeated and the Oregon motion was passed as I reported last week.
Desperate hyperbole
Schadenberg and Russell then desperately argue that you can only support or oppose assisted dying. There is no neutral, they say.
In the language of 'influence' we call this rhetoric "the sucker's choice." You put up just two options and demand folks pick one or the other.
"You're either for us or agin us!"
No other options, no nuances, no consideration of different options for different folks. Hardly the kind of stuff that would pass even a junior high school debate.
Back to the real world
Of course it's possible to be neutral.
Individually, a doctor may be personally opposed to assisted dying, but appreciate that another doctor, having equally examined their conscience, may support choice. Thus, the first doctor opposes for themselves but remains neutral to the position of other doctors. Indeed, an individual doctor may neither support nor oppose choice.
Collectively, it makes sense for a professional medical body to hold a neutral stance. How can it justify respecting the deeply-held beliefs and values of some of its members at the same time as explicitly disrespecting other members' views that are as closely examined and deeply held?
Conclusion
The best that opponents running the global charge against assisted dying can do is to first get their facts wrong (again), develop their false assumptions into shrill hyperbole, and then try to press the false dichotomy of a "suckers choice" into doing some heavy lifting: an exercise that falls flat on its face.
The evidence is crystal clear: they provide no real argument at all.
Blog by Neil FrancisPosted on Thursday 12th May 2016 at 4:30pm
The more anti-euthanasia campaigner Mr Wesley Smith publishes, the more I think he’s missed his true vocation as a comedian. His latest comical gig against assisted dying is a gem.
Mr Smith starts with the case of two Californian doctors found guilty of Medicare fraud: billing fake hospice care for patients who weren't terminally ill. He artfully turns the story into a series of anti-assisted-dying gags.
Who’s on first, What’s on second?
Mr Smith directly connects the money-grabbing fraud case with the Obama administration, ribbing us that the President and federal authorities won’t hold doctors accountable for breaking assisted suicide law. Mr Smith, an attorney, is holding his breath to see if his audience figures out this little joke: oh, the confused jurisdiction names… right!
The Death With Dignity laws are State laws. If the law is broken it is State responsibility to pursue and prosecute offenders. The Feds have no jurisdiction. If, however, Medicare has been defrauded then it’s a Federal matter (FBI): and the Feds did indeed investigate and prosecute.
It’s a bit like the Laurel and Hardy confused “Who’s on first, What’s on second” name sketch, isn’t it? But only if you get it. Grin.
I say, I say, I say: what’s worse—being evil or being dead?
Mr Smith then refers to the case of Michael Freeland, an Oregonian dying of lung cancer who considered using the Death With Dignity Act. Citing himself and referring to the physician who prescribed lethal medication, Mr Smith compares Dr Peter Reagan with the Medicare fraudsters, saying that Dr Reagan “regularly takes on patients solely for the purpose of facilitating their suicides.”
Defamation is always good for a cackle. It’s so droll, like saying that Mr Smith “opposes assisted dying solely because of the great value of redemptive suffering whether others agree or not.” Which, of course, your dear writer is not saying (because Mr Smith has already stated on the record that he doesn't think suffering is redemptive).I’m just saying, you know, for laughs.
Wesley Smith jokes that Dr Peter Reagan is both evil and dead.
To add even greater mirth, Mr Smith describes Dr Reagan as “now late”. OMG, I've met Dr Reagan and he’s a top fellow. He’s died!? No, he hasn't. Fortunately, like Mark Twain, Dr Reagan happily reports that news of his death has been greatly exaggerated.
Phew, comic relief—what a hoot.
The Clause you have when you’re not having a Clause
Mr Smith then tells the one about how doctors ordinarily have to comply with an accepted medical “standard of care,” but that “death doctors” (love those stereotypes, chuckle!) only have to act in “good faith,” which, Mr Smith razzes us, is quite hard to assess. Oh. Awkward audience silence; a cricket chirps. Um, punchline please?
You have to supply your own punchline for this quip I’m afraid, because Mr Smith rather absent-mindedly forgets to. The Oregon Death With Dignity Act 1997 says explicitly in Clause 126.885 §4.01(7), “No provision [of this Act] shall be construed to allow a lower standard of care…”
Ah, more comic relief: the old 'pull-the-wool-over-your-eyes' caper, chortle.
The flip-flop routine
But the most comical gag is the one I reckon Mr Smith doesn’t even realise he’s told: the joke that we’re all going to die from lethal prescriptions, artfully developed by featuring someone he carefully points out didn’t take the lethal prescription. We just love a good flip-flop. LOL.
Oh, that and teasing us that the Medicare fraud case in which the purpose was to get more money is a great story against assisted dying whose purpose, he banters, is to get less (save) money. Double flip-flop: Ta-ching!
Blog by Neil FrancisPosted on Wednesday 27th April 2016 at 11:36pm
Wesley Smith never seems to tire of spreading opinion. In another piece of published nonsense, he's proposed that USA's rise in national suicide rate is in significant part a consequence of assisted dying law in those few states that permit it (up until the most recent general suicide data that's Oregon, Washington state, Vermont and Montana). His claim flies in the face of actual evidence.
Wesley Smith is a Senior Fellow at the Discovery Institute. Remember that? It's the organisation that a USA Federal court ruled pursues "demonstrably religious, cultural, and legal missions," and which comprehensively lost a test case in which it tried to have 'intelligent design' (that's creationism with lipstick) taught as a 'scientific' alternative to evolution.
In a piece recently published by conservative blog NationalReview and reprinted in pro-life LifeSiteNews, Mr Smith has asserted that assisted suicide has a significant part to play in the rising USA national suicide rate. "Color me decidedly not surprised. We are becoming a pro-suicide culture," he asserts.
"I am convinced that the correlation [between assisted suicide advocacy and the general suicide rate] could also be at least a partial causation."
On the matter of rhetoric, notice how Mr Smith cleverly mixes certainty ('convinced') with uncertainty ('could') in order to hedge his literal argumentative bets while giving the impression of valid authority. Ultimately, however, being certain about uncertainty can only be... uncertain.
Mr Smith argues from a USA Centers for Disease Control (CDC) report that the national suicide rate increased more after 2006, "the very time when the assisted suicide movement has become the most vigorous and made its most dramatic advances [emphasis is Smith's]." He offers not one shred of quantitative empirical evidence to support his contention that the assisted dying movement's 'vigor' changed suddenly and substantially from 2006.
So, what does analysis of relevant and readily-available data show? I've reproduced the USA national general suicide rates obtained from the USA government's CDC online database, plus unemployment rates obtained from the USA government Bureau of Labor Statistics online database in Figure 1. (The suicide data does not include deaths under state Death With Dignity Acts because under these Acts such deaths are not suicides.)
Figure 1: USA national suicide and unemployment rates
The national annual suicide rates are shown in red, and the unemployment rates are shown in blue with linear regression lines for before and after 2006. It's easy to see that prior to 2006 the unemployment rate peaked at around 6%, while after 2006—and clearly in response to the global financial crisis (GFC)—the rate peaks much higher at nearly 10%.
Suicide is indeed a complex phenomenon, with a wide range of both risk factors (e.g. unemployment, mental illness, substance abuse) and protective factors (e.g. mental illness mitigation programs, unemployment benefits), and it would be glib to assert only one or a few factors. Nevertheless, Figure 1 demonstrates a clear correlation between trends in unemployment and the overall suicide rate.
Correlation is of course not causation: though I will in a future report show how extensively common this correlation is around the world and over time. Nevertheless, the data, had Mr Smith bothered looking for it, offers a vastly more rational and compelling explanation of the rise in suicide rate than does some hokey theory about how just 325 rational adults in two states (Oregon and Washington state Death With Dignity Act deaths in 2014) who were already dying and quietly and privately chose to go a little early in response to intolerable suffering, caused the suicide rate amongst 319 million inhabitants (2014) across a nation of fifty states, to rise by a "huge and alarming" amount.
Mr Smith backhandedly acknowledges that there are multiple causes of suicide. "There is no question that assisted suicide advocacy is not the only factor causing this alarming increase in suicides," he says, presumptively positioning his hypothetical reason as definitely one of them.
Mr Smith does refer to a recent journal article by David Jones and David Paton that purports to show a weak link between assisted dying and the total suicide rate (with the weak link appearing only if assisted deaths are counted as suicides). I have analysed that paper in detail and shall deal with it in due course. How it passed peer review (if it was indeed peer reviewed) remains a mystery. The study is of an unacceptably poor standard on a range of facets as I will demonstrate.
In conclusion, did the CDC report that Mr Smith cites suggest that 'assisted suicide contagion' was a possible cause of the increase? Nope.
It's really time that Mr Smith and colleagues gave the misinformation campaign a rest.
Blog by Neil FrancisPosted on Sunday 24th April 2016 at 8:02am
The Sydney Morning Herald opinion piece by Dr Andrew McGee
Dr Andrew McGee, Senior Lecturer in law at Queensland University of Technology, published an opinion piece, "Why Bob Hawke is wrong about euthanasia," opposing assisted dying law reform in the Sydney Morning Herald on the 19th April. He invokes straw-man arguments and conflates different issues.
His ‘they might choose to die too early’ argument overlooks both the current tragedy of the terminally ill suiciding by violent means, as well as that in currently lawful jurisdictions like Oregon and Washington, a third of people who qualify for their medication never take it: it provides strong psychological relief that there is another option available whether they take it or not.
His argument that any boundary in regard to who may qualify would be arbitrary is to overlook the intrinsic boundary-ness of law. A minor (under 18) cannot lawfully buy alcohol. A person may not lawfully participate in ‘sophisticated’ investments unless they earn more than $250k a year. We accept legal boundaries as normal and necessary even if some feel a particular boundary is arbitrary. Necessarily, some will be excluded.
Further, arguing against assisted dying law reform on the principle that it’s ‘complicated’ is to argue against law in any case of alleged complexity. Marriage and divorce are complicated. Should we outlaw those?
Dr McGee’s arguments lack coherence and consistency and comprehensively fail to mount a persuasive case against the legalisation of assisted dying.





 Figures 1 and 2 (of Mr Mulino’s minority report): Assisted deaths in Belgium and the Netherlands
Figures 1 and 2 (of Mr Mulino’s minority report): Assisted deaths in Belgium and the Netherlands Figure 3: The full Netherlands data
Figure 3: The full Netherlands data Figure 4: Rate of assisted dying as a percent off all deaths in the Netherlands and Belgium 2003–2015
Figure 4: Rate of assisted dying as a percent off all deaths in the Netherlands and Belgium 2003–2015 Figure 5: Rate of assisted dying in the three lawful Benelux countries
Figure 5: Rate of assisted dying in the three lawful Benelux countries Figure 6: Netherlands total and assisted deaths for different periods
Figure 6: Netherlands total and assisted deaths for different periods Figure 7: The paper Abstract articulates exactly the opposite of Mr Mulino’s claim
Figure 7: The paper Abstract articulates exactly the opposite of Mr Mulino’s claim Figure 8: Table 2 from the 2003 study Mr Mulino cites
Figure 8: Table 2 from the 2003 study Mr Mulino cites Figure 9: Longitudinal NVE rates in the Netherlands, Belgium and the UK
Figure 9: Longitudinal NVE rates in the Netherlands, Belgium and the UK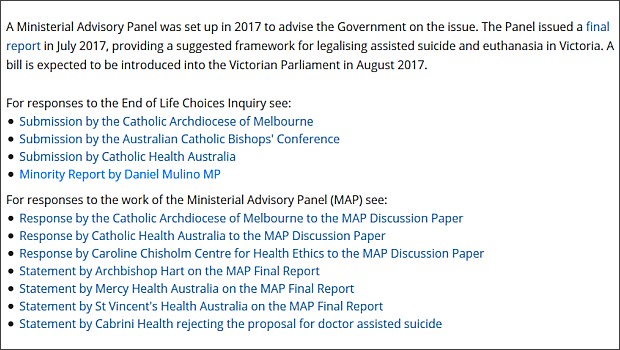 Figure 10: Daniel Mulino’s minority report appears amongst Catholic responses on the Catholic Archdiocese of Melbourne’s website19
Figure 10: Daniel Mulino’s minority report appears amongst Catholic responses on the Catholic Archdiocese of Melbourne’s website19
 Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Figure 1: The Belgium general suicide rate before and after assisted dying law reform