The F filesPosted on Monday 8th August 2016 at 7:02am
Back in 2013 the High Court of Ireland rejected a legal bid by multiple sclerosis sufferer Marie Fleming to achieve a lawfully-assisted peaceful death.
The Court naturally relied on expert testimony in reaching its judgement, yet its conclusions included a statement containing significant errors of fact.
The erroneous statement
In its judgement,1 the Court made the following statement:
“Above all, the fact that the number of LAWER (“legally assisted deaths without explicit request”) cases remains strikingly high in jurisdictions which have liberalised their law on assisted suicide (Switzerland, Netherlands and Belgium) — ranging from 0.4% to over 1% of all deaths in these jurisdictions according to the latest figures — without any obvious official response speaks for itself as to the risks involved.” [My emphases in bold]
In fact, the Court's judgement is wrong on not one, not two, but three significant matters. But that hasn't stopped opponents of assisted dying law reform from quoting the judgement as though it were factual and persuasive, when it isn't: relying on it because it was made by a High Court—the 'authority bias.'
Consequences
Here are just a few examples of the Court's statement being wielded by assisted dying opponents as though it were conclusive evidence against law reform:
Family First’s submission opposing assisted dying law reform in New Zealand.
Catholic lobbyist Paul Russell and Catholic NSW MP Greg Donnelly in submissions to the Victorian (Australia) Parliament inquiry into end-of-life choices.
Catholic Professor Margaret Somerville in the New England Journal of Medicine,2 repeated by Alex Schadenberg of the Euthanasia Prevention Coalition as well as by Catholic-founded National Right To Life News; and Somerville again in the (Catholic) Newman Rambler.3
These examples illustrate the frequency of quoting the misinformation and how it feeds into and wrongly shapes public policy formation.
Three strikes
So what are the three counts on which the Court's judgement was seriously wrong?
Strike 1: Wrong concept
First, let’s get the concepts right. LAWER is not “legally assisted deaths without explicit request.”
Such nomenclature is an oxymoron. To ‘assist’ is to accommodate, serve or help someone accomplish something. But if there has been no request then one cannot be helping. You can’t ‘assist’ a little old lady across the road if she has expressed no interest in going there: you’d be forcing her across the road. Equally, you can’t ‘assist’ a death if there’s no proper ‘request.’
LAWER in fact stands for “Life-ending Acts Without Explicit Request” (of a competent patient).5 And with the exception of the possible ‘lawfulness’ of the doctrine of double effect, such acts are illegal.
Further, if such acts were legal as the Court’s statement posits, then there would be no need for an “obvious official response” as the Court then concludes. The statement lacks fundamental coherence.
Strike 2: Not ‘strikingly high’
The Court's judgement states unequivocally that LAWER (otherwise known as Non-Voluntary Euthanasia or NVE) rates in Switzerland, the Netherlands and Belgium are ‘strikingly high’, though no comparative yardstick is recorded in the judgement by which one might draw or justify that subjective judgement. Similar 'strikingly high' statements also appear in sections 102 and 104 of the judgement.
There is in fact a scientific study, published in The Lancet in 2003, that provides sound empirical evidence that could have properly informed the Court (Figure 1).6
Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002
As revealed by this study, the NVE rates in Switzerland and the Netherlands were in fact lower than in Denmark, a country which has never had an assisted dying law.
The only country which did appear to have an NVE rate notably higher than the others was Belgium. The research study collected the data for analysis between June 2001 and February 2002. However, Belgium’s Euthanasia Act was not passed by its Parliament until 28th May 2002, well after data collection was complete. Thus, even in describing Belgium’s NVE rate as ‘strikingly high’ compared to a number of other European countries, it cannot be attributed to an assisted dying law because none existed at the time.
In fact, the NVE rate in Belgium had been found to be high back in 1998,7 well before the Bill for the country's Euthanasia Act was even tabled in Parliament.
Further, if assisted dying laws had such effects, it might be expected that the NVE rate would increase the longer that assisted dying laws were in place. In that case the NVE rates in Switzerland (statute since 1942) and the Netherlands (regulation since the early 1980s) would have NVE rates much higher than Belgium’s (statute since 2002). But the exact opposite is true.
Indeed, Rietjens and colleagues8 further concluded in their review of NVE in the Netherlands, Belgium, Denmark and Switzerland that “the use of drugs with the intention to hasten death without an explicit request of the patient is part of medical end-of-life practice in the studied countries, regardless of their legal framework, and it occurs in similar fashion.” The study, published in 2007, would also have been important evidence before the Court.
Strike 3: Not ‘remaining’ high
The Court's judgement states unequivocally that the LAWER (NVE) rate of the three countries ‘remains’ strikingly high. No specific evidence was supplied in the judgement to support this statement. Indeed, the judgement notes:
In section 28 that Dutch NVE had been “consistently declining.”
In section 91 that “the number of LAWER deaths has significantly declined in both [Dutch and Belgian] jurisdictions.”
In section 94 that “the trend in [Dutch] LAWER cases are declining in numbers (from 1,000 in 1990 to 550 in 2005)” and that in Belgium “the number of LAWER cases has declined since legalisation of assisted death.”
In section 101 that the NVE rates of both the Netherlands and Belgium had dropped.
Despite this clear and repeated evidence, the Court summarises in section 96 that the evidence cannot be “regarded as encouraging or satisfactory.”
But what does empirical research tell us about the NVE trends? In both the Netherlands and Belgium, since assisted dying was enshrined in statute and became effective in 2002, the rate of NVE has decreased significantly (Figure 2).7,9-11 In fact, the rate in the Netherlands is now similar to that in the UK, a country which has never had an assisted dying law and which provides the world’s gold standard in palliative care practice.
Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying
These are critical yardsticks by which to judge practice in jurisdictions that have assisted dying laws with jurisdictions that don't. The UK study was published in 2009 and was readily available prior to the High Court’s hearings, yet appears not to have been presented in evidence.
The final (2010) Dutch NVE statistic in Figure 2 may or may not have been available to the Court: it was published in 2012 around the time the Court was taking evidence. The final (2013) Belgian statistic would not have been available to the Court as it was published in 2015.
Conclusion
While the High Court worked diligently within the scope of evidence brought before it:
The Court’s definition of LAWER is incorrect and incoherent;
Its statement that the NVE rates of the Netherlands and Switzerland are ‘strikingly high’ are evidentially wrong when compared with other countries without assisted dying laws;
Its implication that the higher NVE rate in Belgium was caused by assisted dying law reform is evidentially wrong; and
Its statement that the rates remain high is evidentially wrong.
The High Court's judgement does not provide defensible evidence or argument against assisted dying law reform.
Many lobbyists have repeated these incorrect statements, significantly misleading media, policy makers and legislators.
Now that the facts are readily available it’s appropriate to avoid repeating evidentially wrong statements, regardless of the apparent 'authority' of their source.
Summary of facts
LAWER stands for "Life-ending Acts Without Explicit Request". Its practice is similar in countries with and without assisted dying laws.
The NVE rates in the Netherlands and Switzerland are lower than the rate in Denmark, a country which has never had an assisted dying law.
The NVE rate in Belgium appears higher, but was so long before assisted dying law reform and so cannot have been caused by such a law.
The NVE rates of the Netherlands and Belgium have both decreased significantly since their assisted dying statutes came into effect in 2002.
References
High Court of Ireland 2013, Fleming v Ireland & Ors - Determination, [2013] IEHC 2, Dublin.
Boudreau, JD, Somerville, MA & Biller-Andorno, N 2013, 'Physician-assisted suicide: should not be permitted/should be permitted', New England Journal of Medicine, 368(15), pp. 1450-1452.
Somerville, M 2016, 'Killing as kindness: The problem of dealing with suffering and death in a secular society', The Newman Rambler, 12(1), pp. 1-26.
Keown, J 2014, 'A right to voluntary euthanasia? Confusion in Canada in Carter', Notre Dame Journal of Law, Ethics & Public Policy, 28(1), pp. 1-45.
Pijnenborg, L, van der Maas, PJ, van Delden, JJM & Looman, CW 1993, 'Life-terminating acts without explicit request of patient', Lancet, 341(8854), pp. 1196-1199.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, 362(9381), pp. 345-350.
Bilsen, J, Cohen, J, Chambaere, K, Pousset, G, Onwuteaka-Philipsen, BD, Mortier, F & Deliens, L 2009, 'Medical end-of-life practices under the euthanasia law in Belgium', New England Journal of Medicine, 361(11), pp. 1119-1121.
Rietjens, JA, Bilsen, J, Fischer, S, Van Der Heide, A, Van Der Maas, PJ, Miccinessi, G, Norup, M, Onwuteaka-Philipsen, BD, Vrakking, AM & Van Der Wal, G 2007, 'Using drugs to end life without an explicit request of the patient', Death Studies, 31(3), Mar, pp. 205-21.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, 23(3), pp. 198-204.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, 380(9845), pp. 908-915.
Chambaere, K, Vander Stichele, R, Mortier, F, Cohen, J & Deliens, L 2015, 'Recent trends in euthanasia and other end-of-life practices in Belgium', N Engl J Med, 372(12), pp. 1179-1181.
Fact file by Neil FrancisPosted on Thursday 7th July 2016 at 10:19pm
Lead author Professor Ezekiel Emanuel discusses the findings of the JAMA study.
Several of the world's foremost researchers in medical end-of-life matters have released a detailed and comprehensive review of the practice of assisted dying in lawful jurisdictions around the world. Published in the Journal of the American Medical Association, it does not support slippery slope hypotheses.
Professors from universities in the USA, the Netherlands and Belgium studied data from government and statutory authority reports, primary scientific studies and other sources to examine how assisted dying has been practiced in different jurisdictions around the world where it is lawful in one form or another: self-administered medication (physician-assisted dying) or physician-administered medication (active voluntary euthanasia).1
Their primary conclusion is that:
"Euthanasia and physician-assisted suicide are increasingly being legalized, remain relatively rare, and primarily involve patients with cancer. Existing data do not indicate widespread abuse of these practices."
Key findings
Key findings include:
Public opinion favouring assisted dying in developed countries has been increasing, or remained stable at high levels of approval.
The trends seem to correlate with decreasing religiosity in Western countries.
The only place where assisted dying approval appears to be decreasing is in eastern Europe, where religiosity has been increasing.
Approval amongst physicians seems to be consistently lower than amongst the public.
Assisted dying occurs everywhere, including juridictions where it is unlawful (as I have previously reported).
Most individuals who choose assisted dying have advanced cancer (as I have previously reported).
Supposedly 'vulnerable' groups are not represented in assisted dying figures at rates any higher than their presence in the overall population.
Numbers of assisted deaths in lawful jurisdictions continue to increase, but represent a tiny minority of deaths.
In jurisdictions where only self-administration is permitted, assisted deaths represent around 0.3% of all deaths.
In jurisdictions where physicians may administer, assisted deaths represent around 3–5% of all deaths.
Assisted deaths for minors and those with dementia are a very small minority of cases (as I have previously reported).
The dominant reasons for requesting assisted death include loss of autonomy and dignity and the inability to enjoy life and regular activities; not physical pain.
Doctors still report that honouring a request for assisted death is emotionally burdensome; not a routine or welcomed option.
"In no jurisdiction was there evidence that vulnerable patients have been receiving euthanasia or physician-assisted suicide at rates higher than those in the general population."
Complication rates
One aspect of the study is worthy of special mention: the small rate of assisted dying procedure complications. The available data suggests that complications may occur more often for self-administered medication than for physician administration:
For self-administration—
Difficulty in swallowing in 9.6% of cases
Vomiting or seizures in 8.8% of cases
Awakening from coma in 12.3% of cases
For physician administration—
Technical problems such as difficulty in finding a suitable vein in 4.5% of cases
Vomiting or seizures in 3.7% of cases
Awakening from coma in 0.9% of cases
This data is however of Dutch practice in the 1990s, before assisted dying was codified in statute—at a time when practice was poorly defined and a range of drugs, including opioids, were widely used. Now, practice is well-defined with almost universal use of barbiturates. The researchers expressly note that these complication rates may well have reduced.
Further, the authors refer to more recent data from Oregon and Washington which indicate very much lower complication rates (in those jurisdictions for self-administration only):
In Oregon, the complication rates are around 2.4% for regurgitation and 0.7% for awakening from coma.
In Washington, the complication rates are around 1.4% for regurgitation, plus a single case of seizure.
The importance of context
It is worth comparing the complication rates of assisted dying procedures with rates for other medical interventions to provide an appropriate context so that they may be realistically interpreted.
For example, a study of common over-the-counter analgesics for short-term pain management2 found that significant adverse effects occurred amongst 13.7% of ibuprofen users, 14.5% of paracetamol useres and 18.7% of aspirin users.
In another example, an anlaysis of primary research about surgical outcomes found that 14.4% had adverse events, almost half of which (47.5%) were moderate to fatal in severity.3
Conclusion
The study is a solid synthesis of research data and indicates that assisted dying is accessed sparingly and in accordance with the intentions of each legislature.
The adverse event rate for assisted dying appears to be substantially lower than the rate of adverse events in the use of common over-the-counter analgesics and in surgery.
References
Emanuel, EJ, Onwuteaka-Philipsen, BD, Urwin, JW & Cohen, J 2016, 'Attitudes and practices of euthanasia and physician-assisted suicide in the united states, canada, and europe', JAMA, 316(1), pp. 79-90.
Moore, N, Ganse, EV, Parc, J-ML, Wall, R, Schneid, H, Farhan, M, Verrière, F & Pelen, F 1999, 'The PAIN Study: Paracetamol, Aspirin and Ibuprofen new tolerability study', Clinical Drug Investigation, 18(2), pp. 89-98.
Anderson, O, Davis, R, Hanna, GB & Vincent, CA 2013, 'Surgical adverse events: a systematic review', Am J Surg, 206(2), pp. 253-62.
Fact file by Neil FrancisPosted on Thursday 28th January 2016 at 1:30am
Around the world, doctors help patients with assisted dying, regardless of whether it is legal in their jurisdiction or not.
For example, in Australia, where assisted dying is illegal, research reveals that assisted dying is widely practiced. Many Australian nurses have collaborated with doctors to provide assisted dying, and have occasionally even done so without consulting a doctor (Kuhse & Singer 1993). Nurses in New Zealand also provide assisted dying, sometimes without consulting a doctor (Malpas, Mitchell & Koschwanez 2015; Mitchell & Owens 2004).
"Euthanasia is common. It's practiced out of sight, under wraps, no regulation, no rules, no supervision." Prof. Peter Baum (Baum 2001)
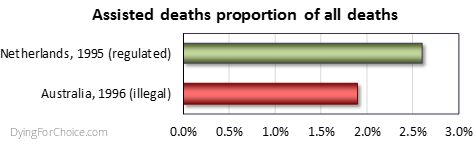
Professor Baum's statement is borne out by scientific research. A national survey of Australian doctors in 1996 found that 1.9% of deaths were the result of voluntary euthanasia (VE) or physician-assisted dying (PAD) (Kuhse et al. 1997). By comparison, the rate in the Netherlands in 1995 (the closest year of empirical research data) was 2.6% (Onwuteaka-Philipsen et al 2012). The rate of medically assisted deaths in Australia, where the practice is illegal, was three quarters the rate of the Netherlands, where the practice is legal.
Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.
Forms of medically assisted dying have been found to occur not only in Australia (and in the Netherlands where it has been lawful for decades), but in Belgium prior to its law reform (Chambaere et al. 2015); Switzerland, Denmark, Sweden and Italy (van der Heide et al. 2003); the UK (Seale 2009a; Seale 2009b); the USA (Back et al. 1996; Bonn 2000; Emanuel, Fairclough & Clarridge 1996; Lachman 2010; Schwarz 2003; Schwarz 2004); France (Riou et al. 2015); Norway (Forde & Aasland 2014; Forde, Aasland & Falkum 1997); and even in conservative Greece (Voultsos, Njau & Vlachou 2010); Northern Ireland (McGlade 2000) and Pakistan (Imran et al. 2014).
Indeed, "euthanasia is performed worldwide, regardless of the existence of laws governing it" (Gastmans et al. 2006), "in all countries studied" (Muller, Kimsma & Van Der Wal 1998), "albeit in a secretive manner" (Rosenfeld 2000), "in the privacy of their [doctor-patient] relationship" (Cassell 1995), with repeated involvement of some physicians (Smith 2007), and frequent failure to adhere to high standards when illegal (Emanuel et al 1998).
Even Dr Brendan Nelson, while President of the Australian Medical Association, acknowledged that he had helped hasten the death of a patient. He stated that in the "2 percent of cases" where there was no hope of recovery, that "patients, their families and their doctors make those decisions [for euthanasia]" though clandestinely, because "technically it would be illegal" (Nelson 1995).
AMA's President, Brendan Nelson, in 1995.
The evidence is irrefutable: there is underground assisted dying worldwide and it demonstrates that there is a profound need for assisted dying law reform to allow dying patients the right to seek a peaceful hastened death, and to protect doctors and nurses who provide that assistance. Law reform would also force assisted dying from the dark shadows, creating transparency and accountability around the process, which would then be open to discussion and improvement if required.
Intolerable and unrelievable patient suffering drives underground assisted dying across the world in jurisdictions where it is illegal, with no standards of practice or transparent oversight.
References
Back, AL, Wallace, JI, Starks, HE & Pearlman, RA 1996, 'Physician-assisted suicide and euthanasia in Washington State: Patient requests and physician responses', JAMA, vol. 275, no. 12, pp. 919-925.
Baum, P 2001, ABC News, TV broadcast 23 Jan, ABC, Sydney.
Bonn, D 2000, 'Support for euthanasia falls as care of dying patients improves', The Lancet Oncology, vol. 1, no. 3, p. 133.
Cassell, EJ 1995, 'Treating the patient's subjective state', Pain Forum, vol. 4, no. 3, pp. 186-188.
Chambaere, K, Vander Stichele, R, Mortier, F, Cohen, J & Deliens, L 2015, 'Recent trends in euthanasia and other end-of-life practices in Belgium', N Engl J Med, vol. 372, no. 12, pp. 1179-1181.
Douglas, C, Kerridge, IH, Rainbird, KJ, McPhee, JR, Hancock, L & Spigelman, AD 2001, 'The intention to hasten death: a survey of attitudes and practices of surgeons in Australia', Medical Journal of Australia, vol. 175, no. 10, pp. 511-515.
Emanuel, EJ, Daniels, ER, Fairclough, DL & Clarridge, BR 1998, 'The practice of euthanasia and physician-assisted suicide in the United States: adherence to proposed safeguards and effects on physicians', JAMA, vol. 280, no. 6, pp. 507-513.
Emanuel, EJ, Fairclough, DL & Clarridge, BR 1996, 'Euthanasia and physician-assisted suicide: Attitudes and experiences of oncology patients, oncologists, and the public', Lancet, vol. 347, no. 9018, pp. 1805-1810.
Forde, R & Aasland, OG 2014, 'Are end-of-life practices in Norway in line with ethics and law?', Acta Anaesthesiol Scand, Aug 14.
Forde, R, Aasland, OG & Falkum, E 1997, 'The ethics of euthanasia -- attitude and practice maong Norwegian physicians', Social Science & Medicine, vol. 45, no. 6, pp. 887-982.
Gastmans, C, Lemiengre, J, van der Wal, G, Schotsmans, P & Dierckx de Casterle, B 2006, 'Prevalence and content of written ethics policies on euthanasia in Catholic healthcare institutions in Belgium (Flanders)', Health Policy, vol. 76, no. 2, pp. 169-78.
Imran, N, Haider, II, Jawaid, M & Mazhar, N 2014, 'Health ethics education: Knowledge, attitudes and practice of healthcare ethics among interns and residents in Pakistan', Journal of Postgraduate Medical Institute, vol. 28, no. 4, pp. 383-389.
Kuhse, H & Singer, P 1993, 'Voluntary euthanasia and the nurse: an Australian survey', International Journal of Nursing Studies, vol. 30, no. 4, pp. 311-322.
Kuhse, H, Singer, P, Baume, P, Clark, M & Rickard, M 1997, 'End-of-life decisions in Australian medical practice', Medical Journal of Australia, vol. 166, no. 4, pp. 191-196.
Lachman, V 2010, 'Physician-assisted suicide: compassionate liberation or murder?', Medsurg nursing : official journal of the Academy of Medical-Surgical Nurses, vol. 19, no. 2, pp. 121-125.
Malpas, P, Mitchell, K & Koschwanez, H 2015, 'End-of-life medical decision making in general practice in New Zealand—13 years on', New Zealand Medical Journal, vol. 128, no. 1418, pp. 27-39.
McGlade, KJ, Slaney, L, Bunting, BP & Gallagher, AG 2000, 'Voluntary euthanasia in Northern Ireland: General practitioners' beliefs, experiences, and actions', British Journal of General Practice, vol. 50, no. 459, pp. 794-797.
Mitchell, K & Owens, G 2004, 'End of life decision-making by New Zealand general practitioners: A national survey', New Zealand Medical Journal, vol. 117, no. 1196, pp. 1-11.
Muller, MT, Kimsma, GK & Van Der Wal, G 1998, 'Euthanasia and assisted suicide: Facts, figures and fancies with special regard to old age', Drugs and Aging, vol. 13, no. 3, pp. 185-191.
Nelson, B 1995, 'Euthanasia a family affair says top doc', The Sunday Territorian, Darwin, 21 May.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Riou, F, Aubry, R, Pontone, S & Pennec, S 2015, 'When physicians report having used medical drugs to deliberately end a patient's life: Findings of the "end-of-life in France" survey', Journal of Pain and Symptom Management, vol. 50, no. 2, pp. 208-215.
Rosenfeld, B 2000, 'Assisted suicide, depression, and the right to die', Psychology, Public Policy, and Law, vol. 6, no. 2, pp. 467-488.
Schwarz, JK 2003, 'Understanding and responding to patients' requests for assistance in dying', Journal of Nursing Scholarship, vol. 35, no. 4, pp. 377-384.
Schwarz, JK 2004, 'Responding to persistent requests for assistance in dying: a phenomenological inquiry', International Journal of Palliative Nursing, vol. 10, no. 5, pp. 225-235.
Seale, C 2009a, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, vol. 23, no. 3, pp. 198-204.
Seale, C 2009b, 'Hastening death in end-of-life care: a survey of doctors', Social Science & Medicine, vol. 69, no. 11, pp. 1659-1666.
Smith, SW 2007, 'Some realism about end of life: The current prohibition and the euthanasia underground', American Journal of Law and Medicine, vol. 33, no. 1, pp. 55-95.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, vol. 362, no. 9381, pp. 345-350.
Voultsos, P, Njau, SN & Vlachou, M 2010, 'The issue of euthanasia in Greece from a legal viewpoint', J Forensic Leg Med, vol. 17, no. 3, pp. 131-6.
Blog by Neil FrancisPosted on Thursday 17th September 2015 at 6:06am
On 16th September 2015, the Victorian Director of the Australian Christian Lobby (ACL), Dan Flynn, appeared as a witness to the Victorian Parliament’s end of life choices inquiry being conducted by the Legal and Social Issues Committee. He made a number of mistaken statements, but what was most worrisome was the revelation of the ACL’s real agenda: to wind back patient rights more than a quarter century.
In his opening address, Mr Flynn opined that assisted dying was 'not supported' by a 'broad base' of Victorian Christians (not just the ACL). This belief is diametrically at odds with clear and repeated evidence from multiple sources.
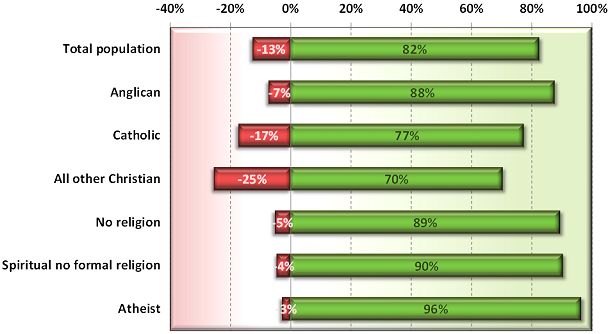
In 2012, I reported on a Newspoll study into Australian attitudes towards assisted dying. Not only did a whopping majority of citizens support assisted dying, but so did a great majority of Anglicans, Catholics and other Christians (Francis 2012).
Newspoll 2012: Australian attitudes to assisted dying law reform by religion (green=support, red=oppose)
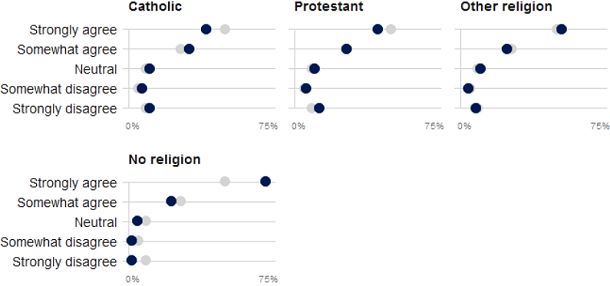
These national results are reflected by a sample of over 60,000 Victorians through the VoteCompass system during the 2014 Victorian election (Stayner 2014). It confirms a substantial majority of Catholics, Protestants, other religious and non-religious Victorians support assisted dying law reform.
VoteCompass 2014: Victorian attitudes to assisted dying law reform by religion (grey=population average)
Out of date
Mr Flynn then referred to a Tasmanian Parliament’s inquiry into assisted dying which rejected law reform. However, the inquiry to which he refers was held in 1998, when Oregon’s Death With Dignity Act had barely been established, the Northern Territory’s Rights of the Terminally Ill Act had been extinguished within just eight months of coming into operation, and the Dutch, Belgian, Luxembourg, Washington and other legislation and judgements did not yet exist.
So, the Tasmanian Parliament’s rejection came from a position of a then general lack of information. The Oregon law has been in effect since 1997, the Netherlands and Belgium since 2002, Washington since 2008, Luxembourg since 2009, and so on. There is now plenty of evidence that assisted dying law reform doesn’t cause slippery slopes that opponents love to theorise about.
Wrong about ‘United Nations’
Mr Flynn then said that the United Nations had in 2012 expressed concern about a ‘lax attitude’ towards euthanasia in Europe, specifically mentioning the Netherlands and Belgium. This is completely untrue. Because it’s easy to make a simple blooper during a presentation, we’ll put aside the fact that he meant to refer to a completely different organisation: the Council of Europe.
We know this because he read directly from Council of Europe declaration 1859 (Council of Europe Parliamentary Assembly 2012). His ACL submission (Australian Christian Lobby 2015) reports (as he read out) exactly one sentence of the declaration, with his added emphasis, as:
"Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited."
But presented in this manner the statement is quite misleading. As I explain in a forensic analysis of the misinformation campaign about this resolution (Francis 2015), the resolution was utterly clear about its intent: it was not about euthanasia (it explicitly said so), but rather about advance care planning. What the resolution spoke against (in the one sentence conveyed above) is non-voluntary euthanasia, not voluntary euthanasia. Both sides of the assisted dying debate agree that non-voluntary euthanasia (one person deciding for a hastened death on behalf of another) is not acceptable. It is not contentious.
In no way did the Council of Europe's resolution critique voluntary euthanasia or comment on any jurisdiction in which it is legal. And, the United Nations source to which the ACL submission refers was released in 2001, fourteen years ago and at the time of the Netherlands' Euthanasia Act was before the Dutch Parliament. With then limited information about how such laws work in practice, it expressed concern about the upcoming Act.
Wrong about Belgium’s law and practice
Mr Flynn referred vaguely to two cases of euthanasia in Belgium in which persons who requested and received euthanasia were not experiencing intolerable pain, which Mr Flynn asserted was a required safeguard in Belgium’s euthanasia Act. This was another supposed example of transgression of safeguards. Wrong again.
While the Belgian Euthanasia Act is officially published only in Dutch and French, a robust English translation has been prepared under the supervision of Professor Herman Nys of the Centre for Biomedical Ethics and Law at the Catholic University of Leuven (see Parliament of Belgium 2002). The word ‘pain’ does not appear in the Act… at all. What does the Act have to say about the legislature’s intent on who may qualify? The relevant clause in Section 1 says:
— "the patient is in a medically futile condition of constant and unbearable physical or mental suffering that can not be alleviated, resulting from a serious and incurable disorder caused by illness or accident."
It’s abundantly clear: mental suffering from an illness or accident qualifies as much as physical suffering, and the suffering does not need to be ‘pain’ as Mr Flynn mistakenly asserted to the Parliamentary Committee.
Mr Flynn also stated that there are mobile end-of-life units in Belgium. There aren’t. (But there are in the Netherlands, and they must follow precisely all the same requirements as anyone else. They operate to provide choice to patients whose regular or reachable doctors disagree with assisted dying and therefore decline to evaluate whether the patient may qualify under the Act.)
Confused about Advance Care Directives
In further testimony, Mr Flynn opined that the degree to which a doctor should be allowed to override a patient’s Advance Care Directive (ACD) is in part influenced by whether the doctor can speak with the patient.
But if the patient can currently speak and participate in decision-making, the advance care directive doesn’t apply: it is mute and of no effect. An ACD only applies when the patient cannot currently participate in their own decision making. That’s (only) what it’s for.
Winding rights back more than a quarter century
But the most worrying aspect Mr Flynn’s testimony was the revelation of ACL’s opposition to the right to refuse unwanted medical treatment.
The Medical Treatment Act 1998 (Vic) has enshrined for now more than twenty five years a patient’s right to refuse any unwanted medical treatments. In 2003 the Supreme Court of Victoria determined that artificial nutrition and hydration (i.e. via tubes) is medical treatment and can therefore be refused under the Act.
But Mr Flynn repeatedly argued that withholding or withdrawing artificial nutrition and hydration, if the patient’s body could ‘absorb’ them, could amount to physician-assisted suicide, and that doctors must be allowed to override refusals. On the matter of patient autonomy, he said that some autonomy rests "with the patients, but a lot of the autonomy in fact is with the doctor”.
When asked if a Jehovah's Witness who refuses a life-saving and simple blood transfusion ought to be allowed to do so, he conceded that they should be entitled to, but that such a case was a “bit of an outlier”. He didn’t explain on what moral grounds one person could refuse a simple procedure to save their life, but another person mustn’t be allowed to even if the likelihood of saving life was doubtful.
So, the ACL’s real agenda is revealed: it recommends winding back the legislative clock more than a quarter century so as to force patients to endure some medical interventions that they don’t want and firmly refuse, if the doctor wishes to proceed.
No wonder the Committee repeatedly questioned Mr Flynn to ensure they had heard and understood his testimony correctly. In conclusion, Committee Chair Edward O’Donohue observed that Mr Flynn’s evidence was “quite surprising” and “quite contrary” to wide evidence already given.
And it’s no wonder that Theo Mackaay, General Secretary of the Victorian Council of Churches—a group of 30 member churches representing mainstream Christianity—criticised the ACL as “fundamentally conservative” and expressed “deep concern that media portrayal of statements from an established and narrow focused lobby group is presented as being representative of the entire Christian community” (Uniting Church in Australia 2011).
-----
References
Australian Christian Lobby 2015, Submission to the Legal and Social Issues Committee on the Inquiry inito End of Life Choices, Parliament of Victoria, Melbourne, pp. 1-17.
Council of Europe Parliamentary Assembly 2012, Resolution 1859 (2012): Protecting human rights and dignity by taking into account previously expressed wishes of patients, Europe, 25 Jan, pp. 2.
Francis, N 2012, Australian public desire for legalisation of assisted dying in restricted circumstances, YourLastRight.com, Melbourne, pp. 11.
Parliament of Belgium 2002, 'The Belgian Act on Euthanasia of May 28th 2002 (unofficial English translation)', Ethical Perspectives, vol. 9, no. 2-3, pp. 182-188.
Uniting Church in Australia 2011, Australian Christian Lobby does not represent all Australian Christians, nor all Christian viewpoints, 8 Dec, Media Room, viewed 11 Dec 2011, <http://blogs.victas.uca.org.au/mediaroom/?p=971>.
 Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002
Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002 Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying
Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying
 Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.
Similarly, Douglas and colleagues (2001) surveyed Australian surgeons, finding that more than a third had provided drugs with the intention to hasten patient death, and with more than half of cases lacking an express request from the patient.