Blog by Neil FrancisPosted on Sunday 6th August 2017 at 2:31am
The terminally ill are not choosing between life and death, but between two ways of dying, according to their own beliefs and conscience. Photo: Andrew Drummond/AAP
In Monday’s Herald Sun, Victorian Archbishops Philip Freier and Denis Hart, and Bishops Ezekiel, Suriel, Lester Briebbenow, Bosco Puthur and Peter Stasiuk published a half-page advertisement admonishing the Victorian government for its initiative to legalise assisted dying for the terminally ill, an ad similar to the one published by religious figures in 2008.
I have no quarrel with individuals of faith regarding their own private beliefs. However, the bishops’ attempt at public “leadership” through the advertisement is deserving of redress for its multiple fallacies.
The ‘abandonment’ fallacy
The bishops claimed that assisted dying “represents the abandonment of those who are in greatest need of our care and support”. On the contrary: to ignore the deeply-held beliefs and rigorously-tested wishes of people at the end of life is to abandon their values and critical faculties in favour of the bishops’ own religious dogma.
The ‘competition’ fallacy
The bishops demand there should be more funding for healthcare rather than assisted dying, fallaciously pitting one option against the other. The Victorian government is indeed increasing funding for palliative care. It’s also aiming to provide lawful assisted dying for when even the best palliative care can’t help – which Palliative Care Australia has acknowledged – giving lie to the faux competition.
The evidential fallacy
Contrary to the bishops’ false presumption that legalised assisted dying will decrease trust in “the treatment and quality of care” from doctors, scientific studies into attitude change show that more people trust doctors when assisted dying is legal. Patients can then talk openly about options, even if they decide against assisted death. The bishops have abandoned facts in favour of religious assumptions.
The equivalence fallacy
The bishops refer to assisted dying as “government endorsed suicide”. They fallaciously equate a reasoned, tested and accompanied decision for a peaceful assisted death in the face of a terminal illness, with the impulsive, violent, isolated and regrettable suicide of individuals (many of whom have mental health and substance abuse issues) who are failing to cope with problems that can be addressed.
However, while the latter are choosing between life and death, the terminally ill are choosing not between life and death, but between two different ways of dying, according to their own beliefs and conscience. Rigorous 2016 research from Australian National University shows that the vast majority (79%) of Victorians support assisted dying choice for the terminally ill (with just 8% opposed), clearly distinguishing it from general suicide.
Shame on the bishops for disrespectfully equating the two.
The inconsistency fallacy
They also argue that assisted dying ought to remain prohibited because within healthcare, “mistakes happen and the vulnerable are exploited,” and “that in spite of our best efforts, our justice system could never guarantee” no one would die by mistake or false evidence. However, as I’ve pointed out before, an identical hypothetical problem exists under the refusal of life-saving medical treatment, a statutory right that Victorians have enjoyed for nearly 30 years. The statute has only three “safeguard” requirements, yet even those only apply if the refusal is formally documented, but not if it’s verbal.
Further, the United States Conference of Catholic Bishops directs that patients may refuse treatment if it imposes “excessive expense on the family or community,” yet makes no mention of the hypothetical “vulnerability” of the patient to be persuaded so, nor directs any requirements to assess the veracity of the refusal.
In stark contrast, the Victorian proposal for assisted dying legislation contains more than 60 safeguards and oversights.
The bishops are at risk of ridicule for such a gargantuan flip-flop: supporting the refusal of life-saving treatment with little or no oversight, while vocally opposing assisted dying legislation that mandates an armada of protections.
The not-so-hidden agenda
The bishops’ methods are rather unsubtle – hoping that these arguments, erroneous but carefully crafted to avoid any religious connotations, will be accepted as non-religious. Yet religion is writ large across their plea: as signatories to the letter they are all clerics employed directly and centrally in the promotion of their religions.
The authority fallacy
They might also rely on their religious status to convey gravity and authority to their pleas. Yet as people paid to do a job, like anyone else, their titles grant them no special privileges in lecturing Victorians about how they should die in the face of a terminal illness.
According to the 2016 census, just 23% of Victorians identified as Catholic, 9% as Anglican, 0.5% as Lutheran, and the other bishops’ signatory denominations so small as to not appear separately in the government’s statistics. Combined, the bishops’ faiths represent around 33% of the Victorian population, while 32% of Victorians identify with no faith at all. Surely the bishops are not arguing that they’re speaking for these other Victorians, too?
But the bishops don’t represent the views of their own flocks, either. According to the 2016 ANU study, 89% of non-religious Victorians support assisted dying law reform, as do 78% of Victorian Catholics and Anglicans. Indeed, opposition to assisted dying exists mostly among those who attend religious services once a week or more often – that is, those who are frequently exposed institutional religious messages of opposition – yet who comprise just 12% of Australians and 11% of Victorians.
Minding their own flocks
Australians are abandoning religion in droves. For example, when Freier ascended to the top job of Anglican Primate of Australia in 2006, some 19% of Australians identified as Anglican (2006 census). A decade later under his leadership, the 2016 census showed a drop of about a third to just 13%, and in Victoria, his home territory, to just 9%.
Hart’s Catholic church has experienced a drop in affiliation too, and it’s likely to continue and accelerate as Australians react with shock and disgust to the extent of child sexual abuse that the royal commission has exposed from under his organisation’s “pastoral umbrella”.
In conclusion, rather than bishops lecturing the government and Victorians with fallacious and faintly desperate arguments about the choices they shouldn’t have at the end of life, attending to their own flocks may be more useful Christian leadership.
May their God go with them in that endeavour.
This article was originally published in The Guardian.
Blog by Neil FrancisPosted on Friday 21st July 2017 at 1:53am
The Parliament of Victoria, Australia
The Victorian Government has introduced its assisted dying Bill into the Victorian Parliament. It's based on extensive consultation with a wide range of stakeholders, and over 1,000 submissions. You can read all about it here.
The Ministerial Advisory Panel on voluntary assisted dying today handed down its final report to the Government.
The Panel was comprised of seven subject experts, with Professor Brian Owler as Chair and Professor Margaret O'Connor as Deputy Chair.
It consulted extensively across Victoria, taking hundreds of submissions and appearances from relevant stakeholders, and reviewing legislation from other jurisdictions in which one form or other of assisted dying is permitted.
Today, it formally handed its report, comprising over 250 pages, to the Government.
The Panel has developed what is arguably the world's most detailed and carefully laid out principles to inform legislation, and are a credit to its efforts and professionalism.
Key aspects of the recommendations for voluntary assisted dying are:
The person must be 18 years or over; and
Be ordinarily resident in Victoria and an Australian citizen or permanent resident; and
Have decision-making capacity in relation to voluntary assisted dying; and
Be diagnosed with an incurable disease, illness or medical condition that:
is advanced, progressive and will cause death; and
is expected to cause death within 12 months; and
is causing suffering that cannot be relieved in a manner the person deems tolerable; and
Doctors and other healthcare workers are not permitted to raise assisted dying — only to respond to formal patient requests.
The person must make three formal requests, the second of which must be written and witnessed by two independent people.
The person must make the request themselves. Nobody else is authorised to make the request, and the request cannot be made via an advance care directive.
Ordinarily, the minimum timeframe between first request and opportunity to take the medication is ten days.
The person must maintain decisional capacity at all three requests.
Two doctors must reach independent assessments that the person qualifies.
Only doctors who have completed specialist training for voluntary assisted dying may participate.
Any healthcare worker may decline to participate for any reason, without penalty.
A prescription dispensed for the purpose of voluntary assisted dying must be kept in a locked box and any unused portion returned to the pharmacy after death.
The person must self-administer the medication; except if the person is unable to, a doctor may administer. An independent witness is required if the doctor administers.
Establishment of an authority to receive assisted dying reports, to assess reports, and to refer unacceptable cases to disciplinary or prosecutorial authorities.
For Parliament to review summary reports; twice in the first two years and annually thereafter; a formal review at five years.
In total, the recommendations include no fewer than 68 safeguards, designed to strike, uniquely for Victoria, an appropriate balance between access to the law, and protection of dying persons.
The Government will respond to the Final Report shortly, and it is anticipated that legislation will be introduced into the Victorian Parliament in August or early September.
A full copy of the Final Report can be obtained here.
-----
Safeguards proposed for Victoria's voluntary assisted dying framework
Access
Voluntary
Limited to 18 years and over
Residency requirement [Victorian resident and Australian citizen or permanent resident]
Limited to those with decision-making capacity
Must be diagnosed with condition that meets restrictive set of criteria [advanced, progressive and will cause death]
End of life is clearly defined [death expected within weeks or months, not more than 12 months]
End of life condition combined with requirement for suffering
All of the eligibility criteria must be met
Mental illness alone does not satisfy the eligibility criteria
Disability alone does not satisfy the eligibility criteria
Request
Must be initiated by the person themselves
No substitute decision makers allowed
Cannot be included as part of an advance directive
Health practitioner prohibited from raising voluntary assisted dying
Person must make three separate requests
Must have written request [witnessed in the presence of a medical practitioner]
Two independent witnesses to request [exclusions for family members, beneficiaries, paid providers]
Specified time must elapse between requests [first and third requests must be at least 10 days apart with exception when death imminent]
Additional time required to elapse between steps of completing process [second assessment and third request must be at least one day apart
Must use independent accredited interpreter [if an interpreter is required]
No obligation to proceed, may withdraw at any time
Assessment
Eligibility and voluntariness assessed by medical practitioners
Must be two separate and independent assessments by medical practitioners
Assessing medical practitioners must have high level of training/experience
Assessing medical practitioners must have undertaken prescribed training [to identify capacity and abuse issues]
Requirement to properly inform person of diagnosis, prognosis and treatment options, palliative care, etc, [by both assessing medical practitioners]
Referral for further independent assessment if there is doubt about decision-making capacity
Coordinating medical practitioner must confirm in writing that they are satisfied that all of the requirements have been met
Medication management
Person required to appoint contact person who will return medication if unused
Medical practitioner must obtain a permit to prescribe the medication to the person
Medication must be labelled for use, safe handling, storage and disposal
Pharmacist also required to inform the person about administration and obligations
Medication must be stored in a locked box
Administration
Medication must be self-administered [except in exceptional circumstances]
If physical incapacity, medical practitioner may administer
Additional certification required if administered by medical practitioner
Witness present if medical practitioner administers
Practitioner protections
Health practitioner may conscientiously object to participating
Explicit protection for health practitioners who are present at time of person self-administering
Explicit protection for health practitioners acting in good faith without negligence within the legislation
Mandatory notification by any health practitioner if another health practitioner acting outside legislation
Voluntary notification by a member of the public of a health practitioner acting outside legislation
Mandatory reporting
Reporting forms set out in legislation
Reporting mandated at a range of points and from a range of participants to support accuracy
First assessment reported [to Board]
Second assessment reported [to Board]
Final certification for authorisation reported [to Board, incorporates written declaration and contact person nomination]
Additional form reported [to Board] if medication administered by medical practitioner
Prescription authorisation reported by DHHS [to Board]
Dispensing of medication reported [to Board]
Return of unused medication to pharmacist reported [to Board]
Death notification data reported [to BDM and collected by Board]
Offences
New offence to induce a person, through dishonesty or undue influence, to request voluntary assisted dying
New offence to induce a person, through dishonesty or undue influence, to self-administer the lethal dose of medication
New offence to falsify records related to voluntary assisted dying
New offence of failing to report on voluntary assisted dying
Existing criminal offences for the crimes of murder and aiding and abetting suicide continue to apply to those who act outside the legislation
Oversight
Guiding principles included in legislation
Board is an independent statutory body
Board functions described in legislation
Board reviews compliance
Board reviews all cases of [and each attempt to access] voluntary assisted dying
Board has referral powers for breaches
Board also has quality assurance and improvement functions
Board has expanded multidisciplinary membership
Board reports to publicly [to Parliament every six months for first two years, thereafter annually
Five year review of the legislation
Guidelines to be developed for supporting implementation
Blog by Neil FrancisPosted on Sunday 5th March 2017 at 10:24pm
Alex Schadenberg's latest shrill and misleading article
Catholic Canadian anti-assisted-dying blogger Alex Schadenberg is at it again. This time he’s parading his ignorance and spreading bull about a potential change in Oregon’s assisted dying legislation.
The Bill
Mr Schadenberg correctly reproduced Section 3 of Oregon Senate Bill 893, which states:
SECTION 3. An expressly identified agent may collect medications dispensed under ORS 127.815 (1)(L)(B)(ii) and administer the medications to the patient in the manner prescribed by the attending physician if:
(1) The patient lawfully executed an advance directive in the manner provided by ORS127.505 to 127.660;
(2) The patient’s advance directive designates the expressly identified agent as the person who is authorized to perform the actions described in this section;
(3) The patient’s advance directive includes an instruction that, if the patient ceases to be capable after medication has been prescribed pursuant to ORS 127.800 to 127.897, the expressly identified agent is authorized to collect and to administer to the patient the prescribed medication;
(4) The medication was prescribed pursuant to ORS 127.800 to 127.897; and
(5) The patient ceases to be capable.
Mr Schadenberg fails to mention Section 2, which states:
SECTION 2. Section 3 of this 2017 Act is added to and made a part of ORS 127.800 to 127.897.
What is the ORS range?
And what precisely is ‘ORS 127.800 to 127.897’ (ORS = Oregon Revised Statutes)? Why, it’s the entirety of Oregon’s existing Death With Dignity Act!
In other words, a patient still has to be terminally ill, fully informed, made a formal request, the request assessed as genuine and free, waited the required cooling off period, made another formal request, been assessed as qualifying all the requirements by multiple doctors, has legally appointed an agent expressly for the purpose of administering lethal medication pursuant to the Death With Dignity Act, have their medication prescribed (immediately before which the attending physician must again verify that the patient is making an informed decision) and then the patient ceases to be capable, before the agent may then administer.
Mr Schadenberg exposes that at best he fundamentally doesn’t understand the Bill, nor took much if any effort to do so.
That’s hardly the free-for-all Mr Schadenberg posits in his shrill blog implying that ‘assisted suicide and euthanasia’ was being extended to ‘incompetent people’ without further qualification; falsely insinuating that any incompetent person could then obtain assistance for suicide or euthanasia.
No ‘defence’
If Mr Schadenberg were to claim that he really meant ‘only within the scope of the current Death With Dignity Act,’ and that he’s been taken out of context, that simply won’t wash. Bill 893 makes a provision only for someone else to administer the lethal dose (that is, what Mr Schadenberg refers to as ‘euthanasia’) if the patient ceases to be capable after already qualifying under the existing Act. The Bill does not permit patient self-administration: that is, using Mr Schadenberg’s own language, ‘assisted suicide’—which he expressly refers to in his article.
Parading a non-existent extension of ‘assisted suicide’ clearly exposes that at best he fundamentally doesn’t understand the Bill, nor took much if any effort to do so.
Wrong again…
He also got it completely wrong as to who may administer when the patient ceases to be capable:
“The bill enables the doctor to administer…” — Alex Schadenberg
However, if you read Section 3 of the Bill (above) that Mr Schadenberg himself reproduces, you’ll see clearly that the patient must expressly identify a particular person ('agent') to administer lethal medication should the patient cease to be capable. The patient may appoint his or her doctor, but can appoint in their Advance Care Directive anyone to be the agent; including a trusted and loved family member. The only particular requirement for the agent’s administration is that he or she must “administer in the manner prescribed by the attending physician.”
Conclusion
But let’s not the facts get in the way of a gratuitous reaction trumpeting shrill hyperbole and headline, shall we Mr Schadenberg?
And as usual, Catholic Australian anti-assisted-dying blogger Paul Russel has dutifully reproduced Mr Schadenberg’s farce.
Blog by Neil FrancisPosted on Thursday 9th February 2017 at 9:53pm
You only have to look to understand who is campaigning against your right to choose an assisted death in the face of intolerable and unrelievable suffering.
A case in point is a massive advertisement published in both of Melbourne’s daily newspapers: News Corp’s The Herald Sun (right-wing) and Fairfax Media’s The Age (left-wing). The ad was published in 2008 when Victorian MLC Colleen Hartland introduced the Medical Treatment (Physician Assisted Dying) Bill into the State legislature.
The Catholic Archbishop of Melbourne, Denis Hart, also sent the advertisement as a letter to all members of the Victorian Parliament.1
So, who are the advertisement’s signatories? I’ve listed them all in Table 1.
Table 1: Signatories to the 2008 Victorian anti-assisted-dying advertisement
Rt Rev. Graham Bradbeer
Moderator, Presbyterian Church of Victoria
The Rev. Fr Graeme A. Michell, FSSM
Parish Priest, Anglican Catholic Parish of St Mary the Virgin, Melbourne
Rev. Ross Carter
Uniting Church in Australia
Pastor Graham Nelson
Senior Pastor, Life Ministry Centre
Rev. Dr Max Champion
National Chair of the Assembly of Confessing Congregations within the Uniting Church in Australia
Rev. David Palmer
Convenor Church and Nation Committee, Presbyterian Church of Victoria
Pastor Mark Conner
Senior Minister of CityLife Church
Rev. Greg Pietsch
President, Victorian District, Lutheran Church of Australia
Dr Denise Cooper-Clarke
Adjunct Lecturer, Ridley Melbourne Mission and Ministry College
Rabbi Dr Shimon Cowen
Director Institute for Judaism and Civilization
Very Rev. Dr Michael Protopopov
Dean - Russian Orthodox Church in Australia
Rev. Megan Curlis-Gibson
St Hilary’s Anglican Church, Kew
Marcia Riordan
Respect Life Office, Catholic Archdiocese of Melbourne
Archbishop Dr Philip Freier
Anglican Church of Melbourne
Metropolitan Archbishop Paul Saliba
Primate of Antiochian Orthodox Archdiocese of Australia, New Zealand & the Philippines
Imam Riad Galil
West Heidelburg Mosque
Member of the Victorian Board of Imams
Bishop Peter Stasiuk CSSR DD
Eparchy of Saints Peter and Paul of Melbourne, for Ukrainian Catholics in Australia and New Zealand
Rev. Father James Grant SSC
Chaplains Without Borders,
Melbourne Anglican Diocese
Dale Stephenson
Senior Pastor Crossway Baptist Church
Assoc. Professor Afif Hadj MB BS (Melb) FRACS
Director of Surgery, Director of Medical Training, Maroondah Hospital (A Monash University Teaching Hospital)
Pastor Peter Stevens
Victorian State Officer
Festival of Light Australia
Archbishop Denis Hart
Catholic Archdiocese of Melbourne
Dr Nicholas Tonti-Filippini
Associate Dean, JPII Institute for Marriage and Family Melbourne
Rev. Fr Geoff Harvey
Priest of the Good Shepherd Antiochian Orthodox Mission Parish, based at Monash University
Rob Ward
Victorian State Director Australian Christian Lobby
Assoc. Professor Rosalie Hudson
Aged Care & Palliative Care consultant/educator
Jim Zubic
President of Orthodox Chaplaincy Association
Peter McHugh
Senior Pastor Christian City Church, Whitehorse
Persons in blue: Career is religion
Almost all of them are religious by career
To save you a lot of time assessing who these people are, I’ve coloured in blue all the folks whose job it is to espouse religion — at least, their own hierarchy’s view of it.
That’s 27 of the 29 signatories who by career are intensely immersed in their own religious perspective of the world; established and promoted through institutional doctrine.
But what about the other two?
What about the other two signatories, Assoc. Prof. Afif Hadi and Assoc. Prof. Rosalie Hudson (in yellow)?
Notice that Prof. Afif Hadi’s entry lists only his surgery profession. Highly relevant, but not mentioned, is that he was President (previously Vice Chairman) of the Australian and New Zealand Board of Trustees, Antiochian Orthodox Archdiocese of Australia and New Zealand. As head of the Board of the Archdiocese, his religious signature is intimately entwined with another: Metropolitan Archbishop Paul Saliba, the Primate of the Antiochian Orthodox Archdiocese.
Assoc. Prof. Rosalie Hudson’s listing too, mentions only seemingly secular links. What is omitted is that she is or was Chair of the University of Divinity (a multi-faith religious institution) Human Research Ethics Committee, Secretary of the Uniting Church’s committee on bioethics, a member of the Interfaith Committee, and an Academic Associate at Charles Sturt University’s School of Theology.
Thus, both Prof. Hadi and Assoc. Prof. Hudson are also deeply rooted in religious faith. The point is not to make any criticism of their faith or practice, but merely to observe the deeply religious connections to opposing assisted dying law reform. It’s worth mentioning that both Hadi and Hudson do valuable charity work.
So, all of them are deeply religious
A pertinent question to ask is: ‘What proportion of the signatories are neutral, scholarly researchers who have studied the empirical evidence from jurisdictions where assisted dying is already lawful?’ Answer: None of them. Enough said.
And what proportion of the signatories to this anti-assisted dying advertisement are very deeply invested in organised religion? The simple answer is as usual: 100%,all of them.
Disconnected from their flocks
Critically, these career-religious fail to reflect the views of their own flocks. We know from repeated polls, for example, that three out of four Australian Catholics, more than three out of four Uniting Church members, and four out of five Anglicans (Church of England) support assisted dying law reform.
This kind of clerical disconnect from the contemporary will of the people is one of the key reasons Australians are deserting religion in droves, as successive censuses show.
Conclusion
The evidence is irrefutable. Those who are actively organised to oppose your right to choose an assisted death are deeply religious, even when they use seemingly secular arguments (more on those later).
They are entitled to their opinions for themselves. But what right do they have to deny the vast majority of Australians, who do not agree with their views, the right to choose?
To phrase it in the personal, why does the Catholic Archbishop of Melbourrne, Denis Hart, think it appropriate to demand that Mr Geoff Drummond, a Buddhist, should have suffered against his will at the end of life for the Archbishop's version of faith, rather than Mr Drummond's own spiritual beliefs? Why does Rabbi Shimon Cowen think it appropriate to demand that Mr Alan Rosendorff, a fellow Jew, should have suffered against his will at the end of life for the Rabbi's version of faith, rather than Mr Rosendorff's own carefully-considered and deeply-held views? And why does Imam Riad Galil think it appropriate to demand that Mr Peter Short, not a Muslim, should have suffered against his will at the end of life for the Imam's beliefs, rather than his own?
Perhaps hubris remains alive and well amongst religious conservatives?
-----
Declaration: In fairness to those mentioned in this article, I openly declare that I am agnostic.
References
Bradbeer, G, Rt Rev., Carter, R, Rev., Champion, M, Rev. Dr, Conner, M, Pastor, Cooper-Clarke, D, Dr, Cowen, S, Rabbi Dr, Curlis-Gibson, M, Rev., Freier, P, Archbishop Dr, Galil, R, Imam, Grant SSC, J, Rev. Fr, Hadj, A, Assoc. Prof., Hart, D, Archbishop, Harvey, G, Rev. Fr, Hudson, R, Assoc. Prof., McHugh, P, Michell, GA, Rev. Fr, Nelson, G, Pastor, Palmer, D, Rev., Pietsch, G, Rev., Pietsch, M, Protopopov, M, Very Rev. Dr, Riordan, M, Saliba, P, Metropolitan Archbishop, Stasiuk, P, Bishop, Stephenson, D, Stevens, P, Pastor, Tonti-Filippini, N, Dr, Ward, R & Zubic, J 2008, Reject physician assisted dying - An open letter to Victorian MPs, Catholic Archdiocese of Melbourne, viewed 13 Jun 2008, http://www.cam.org.au/Euthanasia.aspx.
Blog by Neil FrancisPosted on Saturday 3rd September 2016 at 1:12am
BMA House in Tavistock Square, London, home to the British Medical Association since 1925.
A meeting has been held at BMA House in Tavistock Square, the home of the British Medical Association since 1925, to discuss assisted dying law reform.1
The meeting, chaired by Lord Moynihan and attended by eminent doctors, dignitaries and the President of the Free Church Council, discussed and voted on the motion:
"That in the interests of humanity it is desirable that voluntary euthanasia subject to adequate safeguards should be legalized for persons desiring it who are suffering from incurable, fatal, and painful disease."
Familiar arguments for and against were proffered by a range of speakers. In addition a range of letters of support and apologies for inability to attend in person were read, from Lord Ponsonby, Sir Frederick Menzies, Sir P. Varrier-Jones, Mr McAdam Eccles, Sir John Robertson, Sir Arnold Wilson MP, Miss Eleanor Rathbone MP, and a small number of well-known clergy.
Rev. Norwood, President of the National Free Church Council, strongly supported the motion.
The motion was put to the vote and passed by a majority of ten to one.
The year? 1935.
The meeting established the Voluntary Euthanasia Legalization Society of the UK.
Subscription to the Society was set at a minimum of five shillings (about £57, US$76 or AUD$100 in today's money), but this was once only and not annually, "for it was hoped the society would soon disappear, owing to the success of its efforts."
Founding members were just a little over-optimistic.
-----
1. Fleming, RA 1935, 'Voluntary Euthanasia', British Medical Journal, vol. 2, no. 3910, p. 1181.
The F filesPosted on Thursday 23rd June 2016 at 7:39pm
Yesterday in a prominent opinion piece in The Age newspaper,1 palliative care specialists argued that palliative care is imperfect and in need of an injection of funds. I agree on both counts.
Nurse Peter Hudson, and doctors Mark Boughey and Jennifer Philip of the Centre for Palliative Care argued that instead of assisted dying as recommended by the recent Victorian Parliament committee report, increased funding of palliative care is ‘the answer.’
Key arguments
Here are the highlights of their opinion piece:
They refer to assisted dying, a neutral expression now in common use amongst both lay commentators and scholars, as a euphemism. Instead they laboriously refer to assisted suicide (suicide is universally seen as a pejorative term with all its baggage about mental illness and substance abuse), and euthanasia (consistently omitting the qualifier ‘voluntary’).
Dying at home should not be the gold standard (despite the great majority preferring it); instead, dying in hospital can be ‘preferred.’
In a profound lack of self-reflection or consistent logic, they say that assisted dying ought to remain outlawed because its outcomes are uncertain. Even assuming the premise of the statement, this would be an identical argument to ban palliative care, whose outcomes are at least equally if not considerably more uncertain.
They falsely imply that users of assisted dying not infrequently experience “very unfavourable” reactions to the drugs. This is simply untrue and I challenge them to provide the empirical evidence that they state is so very important.
Tellingly, they describe a peaceful assisted death as “sanitised,” signalling their intrinsic disapproval of other’s choices.
They say that focus should remain on increased resourcing of palliative care, failing to mention that the Parliamentary committee’s report indeed recommended increases in palliative care funding and improvement of evidence-based practice. Overseas evidence also reveals improvements in palliative care in jurisdictions with assisted dying legislation. There’s no false dichotomy between palliative care and assisted dying as the authors try to insinuate.
They assume that medical interventionism (what they have to offer) is the correct and normative response, ignoring the fact that some people simply don’t want more interventions.
The filibuster
In a journal article recently published by two of the opinion piece authors,2 and repeated in principle in the Centre’s submission to and appearance before the Parliamentary inquiry,3,4 they say that:
“Increased resources and effort must be directed toward training, research, community engagement, and ensuring adequate resourcing for palliative care to benefit many before further consideration is given to allocating resources into legalising EAS to respond to the requests of a few.”
Notice two things about their recommendation—the filibuster.
Maximising what cannot be done
Firstly, they say we must not just ban assisted dying, but that it is dangerous even to talk about it: palliative care must be improved even “before further consideration is given.” The specific purpose of this part of the filibuster is to maximise what cannot be done: to position even mere conversation, let alone actual reform, as ‘unsafe.’
Maximising the delay
Secondly, nowhere in their argument do they provide a single quantitative metric (and which they strongly argue is necessary for the legalisation of assisted dying) by which the palliative care reforms they advocate might be judged: not a single dollar amount nor a single performance benchmark amongst their many recommendations.
How much will reforms cost, how long will they take, and what performance measure improvements would need to be achieved for the expenditure to be judged effective? What performance measures would need to be reached before it was then ‘safe’ to even consider assisted dying? The authors are entirely mute on these critical matters, while making precisely these evidential demands of assisted dying.
So, the opinionists’ argument allows them to indefinitely say that “more improvements are needed in palliative care before we even talk about assisted dying,” because further ‘improvements’ are always possible.
But all that was a ruse anyhow
In any case, the authors say in their submission to the Parliamentary inquiry that there are numerous problems (spurious, I argue) with legalising assisted dying; that they doubt they could be overcome; and then finally “it should not be construed that we would support the legalisation of EAS if efforts were made to address [the problems].”4, page 6 (Curiously, they omit the third, critical statement from their more public opinion piece.)
This truly exposes the classic filibuster… an open-ended call with no metrics, which therefore can be deemed never to have been met. How convenient. But, even if they were met, the authors still wouldn’t support reform. This begs the question:
If the authors are as so firmly evidence-based—as they take pains to emphasise—why would they not support a reform if the evidence endorsed it?
There must be something other than evidence that drives their entrenched opposition to assisted dying: something so important that it renders all their previous arguments null and void. What might that be?
Who are these people, anyway?
It’s informative to answer the question of who these three from the Centre for Palliative Care are. The Centre sounds like a neutral government body. It isn’t. Don’t get me wrong. I have no doubt that these three are skilled and compassionate practitioners and that the Centre delivers good services.
In reality the Center is a section of Melbourne’s St Vincent’s Hospital. That’s an organisation that proudly states “as a Catholic healthcare service we bring God’s love to those in need through the healing ministry of Jesus.”
I believe St V’s to be a high-quality healthcare institution, but too bad if the patient just wants evidence-based medical care and not the ‘healing ministry’ of a religious figure they may not subscribe to.
The reason this is important is this: what the three authors say about assisted dying is entirely consistent with the Vatican’s stance. I have no idea if any of the authors are Catholic, but what would be entirely surprising is if they published anything at odds with the views of the Vatican given their Centre is deeply embedded within the largest Catholic health and aged care service provider in the country.
For clarity and fairness, I once again place on the public record that I am agnostic.
The ‘Catholic card’
Before Messers Paul Russell, Alex Schadenberg and others leap onto their campaigning steeds to megaphone that I’m ‘playing the Catholic card’ (just wait for it!), let me be clear that I specifically am doing precisely that. For sure, The Catholic Church is not the only religious body resolutely opposed to anyone having the choice of assisted dying, but it’s the premier one.
And, Messers Russell et al would be absolutely right to point out that the authors didn’t raise a single religious argument, so let me save them the bother.
Religious opposition dressed up in secular garb
And that’s the point. It’s abundantly clear from multiple sources that religious opponents have actively decided that they will absolutely avoid using religious arguments because they know it will lose them the debate.
Media identity Andrew Denton’s Better Off Dead podcast series makes this avoidance abundantly clear from the Australian perspective. His insights, having attended a global anti-euthanasia conference in Adelaide, are important and revealing.
From the North American perspective, a study just published by Associate Professor Ari Gandsman of the University of Ottawa in Death Studies5 reports uncanny North American similarities. Assisted dying opponents have actively decided to cease using religious arguments. Instead, their objective is to create an atmosphere of FUD: fear, uncertainty and doubt. It is only this now, they agree amongst themselves, that will keep assisted dying off the statute books. As Gandsman explains (and I paraphrase), religious opponents have moved from ‘it’s a sin’ to ‘but think about all the perceived risks!’
Again, I reiterate that the three opinion piece authors are likely to be fine nurses and doctors (I have never met any of them), but I do say that their incoherent and self-contradictory arguments against assisted dying, remaining opposed even ‘if’ the evidence for it stacks up, is neither their finest work, nor varies one iota from the religious anchor that the Vatican provides to their Centre’s services.
The importance of mutual respect
If a person says to me “I believe assisted dying is wrong,” I respect that view and admire their resolution. For themselves. Including if it is underpinned by religious belief. If you believe that assisted dying, or surrogacy, or other contentious issue is wrong, don’t participate in it.
But don’t expect that your own view of your own God trumps everyone else’s God—or lack thereof. In Australia for example, the majority of citizens are not Catholic. And most of those who are—three out of four—disagree with the Vatican’s opposition to assisted dying. The Vatican’s view then is not particularly relevant to anyone but its most ardent adherents.
Respect in both directions is warranted but is rather lacking from the more religious end. My argument is not against Catholicism itself. There are very fine Catholics on both sides of the debate, doing their best to live a deliberatively ‘good’ life.
Conclusion
We can do without the incoherent and indefensible nonsense advanced in secular garb by the religiously opposed.
Be clear folks: the FUD campaign is on its last legs. I will be further exposing rubbish arguments posed by those with religious connections but couched in non-religious language.
In the meantime you can see the clumsy, failed attempt at a filibuster by these three opinionists for what it is.
References
Hudson, P., Boughey, M. & Philip, J., 2016, Victoria's proposed euthanasia laws are flawed, Melbourne: Fairfax Media, Accessed 21 Jun 2016, http://www.theage.com.au/comment/victorias-proposed-euthanasia-laws-are-flawed-20160620-gpn9p2.html
Hudson, P., Hudson, R., Philip, J., Boughey, M., Kelly, B. & Hertogh, C., 2015, Legalizing physician-assisted suicide and/or euthanasia: Pragmatic implications for palliative care, Palliative and Supportive Care, 13(5), 1399-1409.
Hudson, P., 2015, Inquiry into end of life choices: Submission 905 to the Parliament of Victoria, Centre for Palliative Care, St Vincent’s Hospital, Melbourne.
Hudson, P., Boughey, M. and Philip, J., 2016, Witness Appearance Transcript: Inquiry into end-of-life choices - Centre for Palliative Care, Parliament of Victoria, Melbourne, 24 Feb.
Gandsman, A., 2016,“A recipe for elder abuse:” From sin to risk in anti-euthanasia activism. Death Studies, In press.
News reportPosted on Sunday 19th June 2016 at 9:03pm
The Canadian Parliament has passed a law that allows the terminally ill to choose assisted dying in restricted circumstances.
The Parliament of Canada has legalised assisted dying. (Photo: Jeffery Nichols)
The historic law was passed this Friday and allows a dying patient to opt for assisted dying within specific limitations:
The patient must —
be 18 or older;
be mentally competent;
be eligible for government-funded healthcare (at the same time as ensuring the patient has access to appropriate care, this prevents non-residents from accessing the law);
Have a serious, incurable illness or condition in an advanced state of irreversible decline; and
Be experiencing intolerable suffering.
The patient's request must be signed by two independent witnesses.
There is a mandatory cooling off period of fifteen days.
Canadian Prime Minister Justin Trudeau supported the legislation.
Jody Wilson-Raybould, Miniter for Justice, issued a statement with the Attorney General and Minister of Health, saying that the legislation as passed "strikes the right balance between personal autonomy for those seeking access to medically assisted dying and protecting the vulnerable."
News reportPosted on Sunday 8th May 2016 at 11:27pm
The Australian Federal election is now officially 'on'. You can take Vote Compass' questionnaire and indicate your views on assisted dying for the terminally ill, amongst other things.
Again this election, Vote Compass is running a service that allows you to explore how your views align with various parties and candidates.
One of the key questions in the Vote Compass repertoir is to agree or disagree with the statement "Terminally ill patients should be able to legally end their own lives with medical assistance."
You can indicate your support for this long-overdue law reform by completing the questions at Vote Compass here.
Blog by Neil FrancisPosted on Sunday 24th April 2016 at 8:02am
The Sydney Morning Herald opinion piece by Dr Andrew McGee
Dr Andrew McGee, Senior Lecturer in law at Queensland University of Technology, published an opinion piece, "Why Bob Hawke is wrong about euthanasia," opposing assisted dying law reform in the Sydney Morning Herald on the 19th April. He invokes straw-man arguments and conflates different issues.
His ‘they might choose to die too early’ argument overlooks both the current tragedy of the terminally ill suiciding by violent means, as well as that in currently lawful jurisdictions like Oregon and Washington, a third of people who qualify for their medication never take it: it provides strong psychological relief that there is another option available whether they take it or not.
His argument that any boundary in regard to who may qualify would be arbitrary is to overlook the intrinsic boundary-ness of law. A minor (under 18) cannot lawfully buy alcohol. A person may not lawfully participate in ‘sophisticated’ investments unless they earn more than $250k a year. We accept legal boundaries as normal and necessary even if some feel a particular boundary is arbitrary. Necessarily, some will be excluded.
Further, arguing against assisted dying law reform on the principle that it’s ‘complicated’ is to argue against law in any case of alleged complexity. Marriage and divorce are complicated. Should we outlaw those?
Dr McGee’s arguments lack coherence and consistency and comprehensively fail to mount a persuasive case against the legalisation of assisted dying.
Blog by Neil FrancisPosted on Sunday 22nd November 2015 at 5:05am
The Parliament of Victoria is conducting an inquiry into end-of-life decision making.
The standing Legal and Social Issues Comittee of the Parliament of Victoria, Australia, is currently conducting an inquiry into end-of-life decision making, to inform any legislative changes required in order to reflect contemprary views and best practice.
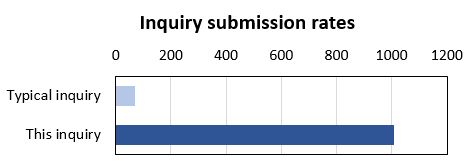
The inquiry has certainly engaged the community: it has received a record number of submissions. The Legal and Social Issues Committee typically receives a couple of dozen submissions to any of its inquiries, occasionally even sixty or eighty. In contrast, the inquiry on end-of-life decision making has received more than one thousand (1,017) submissions.
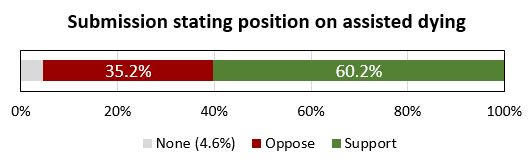
Most of the submissions (98%), including DyingForChoice.com's, are published on the Committee's website, with the tiny remainder kept confidential at the request of the submitter.
The terms of reference for the inquiry are completely silent on the matter of assisted dying. The Terms talk about "making informed decisions", "exercising preferences" and "the role of palliative care" in the context of current legislation and any required changes.
So, given that assisted dying is not mentioned in the Terms of Reference, you'd expect a modest number of submissions to address the issue, right? Wrong.
Of the submissions that are published on the Committee's website (and which I could therefore read), a staggering 95.4% of them make specific and deliberate points about assisted dying law reform, and 60.2% of the published submissions make points in favour of law reform to permit assisted dying in one form or another.
There is no clearer indication than this of how deeply engaged the Victorian public is with end-of-life decision making, and how important assisted dying law reform is to the options they might consider.
The Leglislative Council and this Committee are to be highly commended for establishing and conducting the inquiry. Public hearings with witness appearances have further helped inform the Committee and its Secretariat. The transcript of my appearance can be read here.
We the people of Victoria look forward with anticipation to the final report of the Committee, and the recommendations it makes. The Committee must report back to the Legislative Council no later than 31st May 2016. But, given the tsunami of submissions and the continuing public hearings, we won't be surprised if the Committee is granted an extension to complete its work.




")