Blog by Neil FrancisPosted on Tuesday 14th June 2016 at 10:22pm
Mrs Inga Peulich of the Victorian Parliament.
Mrs Inga Peulich is MLC for the Victorian state region of South-Eastern Metropolitan and is Shadow Minister for Multicultural Affairs and for Scrutiny of Government. She is a member of the Parliament's Legal and Social Issues Committee, which recently recommended assisted dying law reform.
She has previously made clear her personal opposition toward assisted dying law reform. It's no surprise then that she wrote a minority report against her own Committee's final recommendations. What is surprising is the incoherence of her report.
They're biased but I'm not
Mrs Peulich rails against the inquiry being held in the first place, saying that she outright opposed the call. It's curious then that she remained on the Committee once the inquiry was mandated by the Legislative Council.
Even more telling is that Mrs Peulich accuses her fellow Parliamentary Committee members of unmitigated bias—that they simply reached a foregone conclusion. Not only does such hubris demonstrate a breathtaking disregard for the dedication and professionalism of her fellow Parliamentarians, it reveals a comprehensive failure of self-reflection: that other members are biased for the possibility of a supportive stance, but she is not for her preset and entrenched opposition.
The criticism is all the more galling for the fact that Mrs Peulich missed a number of meetings to hear from expert witnesses. Other members were informed and their position changed or at least nuanced by the evidence and advice.
The ramble
Mrs Peulich's minority report then launches into a ramble of conjecture, raising many of the tired old discredited arguments against assisted dying without reference to a single cited fact; incoherently even making points that the Committees' final report (hundreds of pages, fully cited) can't support...and ones that I specifically, comprehensively and evidentially refuted in my submission to and expert witness appearance before the Committee.
At least one appropriate omission
I can say that in response to a question Mrs Peulich asked me about non-voluntary euthanasia in the Netherlands, in what she might have anticipated as a 'gotcha' moment, I used empirical scientific evidence to blast the premise of her question—that legalisation of voluntary euthanasia has increased the rate of Dutch non-voluntary euthanasia—out of the water. The rate has dropped dramatically, not increased. At least she didn't raise that hoary old Dutch chestnut directly in her report.
Selective perfectionism
It would be tedious to address every item of unsupported conjecture and misinformation in Mrs Peulich's report. However, one other claim is worthy of discussion. It's an argument she's made before. She says this in regard to assisted dying law reform:
"...people will die as a result of accident, error or misdiagnosis. Any accidental loss of life – even the loss of one life, means such a regime cannot be justified."
Putting aside for the moment the premise of the statement, Mrs Peulich's selectivity is remarkable.
Published scientific research shows that of hospital admissions (Australia), around 0.4% result in death as a consequence of preventable medical error.1 The study was published some twenty years ago, so let's assume that the error rate has dropped—by virtue of greatly improved record keeping, communication, transparency, procedures and technology since then—by a factor of ten: that is, a preventable medical error death rate of 0.04%.
That still means that at least dozens of Victorians die each year as a result of preventable medical error.
If Mrs Peulich argues that no system can be justified if it results in the erroneous loss of a single life, then she must equally argue for the closure and prohibition of the entire Victorian hospital system. Or admit that she's irrationally biased against the option of assisted dying.
Missing critical Oregon 'information'
Yet the most telling thing is what is missing from Mrs Peulich's minority report.
On April 8th 2010, as keynote speaker and in her capacity as member of the Victorian Parliament, at Australian Catholic University's Interfaith Symposium on Death and Dying, she made this unequivocal statement:
"The Oregon experience, which legislated the taking of medication to bring about euthanasia indicates unfortunately that it does occur, that older patients who are tapping into more expensive care are encouraged often to bring about their own earlier demise."
Such a situation would be a very, very serious matter indeed.
But did Mrs Peulich furnish any evidence to support her allegation? No, none whatsoever.
If she believes this matter to be true, and it would be of critical importance to the inquiry to which she was directly a party and would strongly support her case against reform, why does it not appear in her minority report?
Mrs Peulich, put up or apologise
The claim is bunkum. Having extensively studied dozens of reports about and scientific studies into practices in Oregon and personally interviewed key Oregonian stakeholders (for, against and neutral), I have found not a shred of evidence that supports Mrs Peulich's categorical assertion.
I expressly challenge Mrs Peulich to furnish the necessary, verifiable, authoritative evidence (not mere self-serving gossip and scuttlebutt), and to explain why it does not appear as evidence to her own Committee's investigation.
If she is unable to provide such evidence or satisfactorily explain its absence from her minority report, it is my view that she owes the people of Victoria an apology for the spreading of misinformation on the taxpayer's tab.
A dead bat to this challenge would only serve to highlight that her claims are rubbish and that this kind of approach deserves no place in the important public discourse about assisted dying.
----------
1. Wilson, Ross McL, Runciman, William B., Gibberd, Robert W., Harrison, Bernadette T., Newby, Liza & Hamilton, John D.. 1995. The Quality in Australian Healthcare Study. Medical Journal of Australia 163: 458-471.
Blog by Neil FrancisPosted on Sunday 8th May 2016 at 9:48pm
Jeanne Smits' completely false statement in LifeSiteNews
Well it didn't take long. Recently I posted a fact-based report card on Dutch euthanasia practice, based on the actual data from the 2015 annual report (and all the earlier reports) of the Dutch Euthanasia Commission. Now, just a few days later, conservative religious opponents have begun publishing completely untrue statements about Dutch euthanasia practice.
Catholic blog LifeSiteNews' 'Paris correspondent' Jeanne Smits has bolted out of the misinformation blocks, assertively and categorically stating in respect of the small increase in number of euthanasia cases from 2014 to 2015, that:
"The rise is mainly due to the increase of euthanasia for demented, elderly people as well as psychiatric patients, two categories that raise even more questions than 'ordinary' euthanasia for untreatable physical pain."
Smits goes on to correctly report that dementia was an underlying factor in 109 of the cases in 2015 (against 81 in 2014) and psychiatric disorders in 56 patients (against 41 in 2014).
The total number of euthanasia cases increased from 5306 in 2014 to 5516 in 2015, an increase of 210 cases. The increase in dementia cases was 28 and in psychiatric disorders was 15. Therefore, underlying dementia accounted for 13% of the increase, and psychiatric disorders 7% of the increase.
Cherry-picking
Smits has cherry-picked just the dementia and psychiatric illness figures and presented them in a way that supports her story arc, painting a bleak picture.
But by no stretch of the imagination does dementia and psychiatric illness account "mainly" for the increase as she categorically states.
What didn't Smits report at all? Cancer: the Netherlands' leading cause of death. In 2015, cancer was the underlying condition in 4000 euthanasia cases, against 3888 in 2014, a rise of 112 cases or 53% of the increase. That compares with dementia at 13% and psychiatric illness at 7% (20% combined), which Smits selectively critiques as a 'sharp rise'.
In no way is Smits' statement true.
No, let's be frank: it's an outright lie. Cancer was the major underlying condition accounting for more than half of the small increase (4%) of cases in 2015.
More evidence refutes the claim
Comparing one years' data with just the preceding years' data can be misleading when the number of observations is low, as it is for dementia and psychiatric illness euthanasia cases. Fortunately, we have data for more than just the one year.
Since 2012 the Euthanasia Commission has consistently published specific figures for dementia and psychiatric illness cases, so we can compare a rise over four years rather than just one. On this basis as a proportion of total 2012 cases, there has been a 17.9% increase in cancer-related cases, a 1.6% increase in dementia cases, and a 1.0% increase in psychiatric illness cases.
Longitudinal data is even more clear than a single year. It unequivocally refutes Smits' silly claim.
Bull is spread
Does Smits' claim matter much? Won't it just slip into oblivion?
No. Michael Haverluck of the conservative Christian paper OneNewsNow has already picked up Smits' article and repeated her claim as gospel. It remains to be seen how many other anti-euthanasia bloggers republish this nonsense.
Unacceptable conduct
In my view, publishing such a categorical yet false statement — even when unintentional — without first properly checking the facts, is unacceptable conduct. The article (and its derivatives) ought to be withdrawn.
Blog by Neil FrancisPosted on Wednesday 27th April 2016 at 11:36pm
Wesley Smith never seems to tire of spreading opinion. In another piece of published nonsense, he's proposed that USA's rise in national suicide rate is in significant part a consequence of assisted dying law in those few states that permit it (up until the most recent general suicide data that's Oregon, Washington state, Vermont and Montana). His claim flies in the face of actual evidence.
Wesley Smith is a Senior Fellow at the Discovery Institute. Remember that? It's the organisation that a USA Federal court ruled pursues "demonstrably religious, cultural, and legal missions," and which comprehensively lost a test case in which it tried to have 'intelligent design' (that's creationism with lipstick) taught as a 'scientific' alternative to evolution.
In a piece recently published by conservative blog NationalReview and reprinted in pro-life LifeSiteNews, Mr Smith has asserted that assisted suicide has a significant part to play in the rising USA national suicide rate. "Color me decidedly not surprised. We are becoming a pro-suicide culture," he asserts.
"I am convinced that the correlation [between assisted suicide advocacy and the general suicide rate] could also be at least a partial causation."
On the matter of rhetoric, notice how Mr Smith cleverly mixes certainty ('convinced') with uncertainty ('could') in order to hedge his literal argumentative bets while giving the impression of valid authority. Ultimately, however, being certain about uncertainty can only be... uncertain.
Mr Smith argues from a USA Centers for Disease Control (CDC) report that the national suicide rate increased more after 2006, "the very time when the assisted suicide movement has become the most vigorous and made its most dramatic advances [emphasis is Smith's]." He offers not one shred of quantitative empirical evidence to support his contention that the assisted dying movement's 'vigor' changed suddenly and substantially from 2006.
So, what does analysis of relevant and readily-available data show? I've reproduced the USA national general suicide rates obtained from the USA government's CDC online database, plus unemployment rates obtained from the USA government Bureau of Labor Statistics online database in Figure 1. (The suicide data does not include deaths under state Death With Dignity Acts because under these Acts such deaths are not suicides.)
Figure 1: USA national suicide and unemployment rates
The national annual suicide rates are shown in red, and the unemployment rates are shown in blue with linear regression lines for before and after 2006. It's easy to see that prior to 2006 the unemployment rate peaked at around 6%, while after 2006—and clearly in response to the global financial crisis (GFC)—the rate peaks much higher at nearly 10%.
Suicide is indeed a complex phenomenon, with a wide range of both risk factors (e.g. unemployment, mental illness, substance abuse) and protective factors (e.g. mental illness mitigation programs, unemployment benefits), and it would be glib to assert only one or a few factors. Nevertheless, Figure 1 demonstrates a clear correlation between trends in unemployment and the overall suicide rate.
Correlation is of course not causation: though I will in a future report show how extensively common this correlation is around the world and over time. Nevertheless, the data, had Mr Smith bothered looking for it, offers a vastly more rational and compelling explanation of the rise in suicide rate than does some hokey theory about how just 325 rational adults in two states (Oregon and Washington state Death With Dignity Act deaths in 2014) who were already dying and quietly and privately chose to go a little early in response to intolerable suffering, caused the suicide rate amongst 319 million inhabitants (2014) across a nation of fifty states, to rise by a "huge and alarming" amount.
Mr Smith backhandedly acknowledges that there are multiple causes of suicide. "There is no question that assisted suicide advocacy is not the only factor causing this alarming increase in suicides," he says, presumptively positioning his hypothetical reason as definitely one of them.
Mr Smith does refer to a recent journal article by David Jones and David Paton that purports to show a weak link between assisted dying and the total suicide rate (with the weak link appearing only if assisted deaths are counted as suicides). I have analysed that paper in detail and shall deal with it in due course. How it passed peer review (if it was indeed peer reviewed) remains a mystery. The study is of an unacceptably poor standard on a range of facets as I will demonstrate.
In conclusion, did the CDC report that Mr Smith cites suggest that 'assisted suicide contagion' was a possible cause of the increase? Nope.
It's really time that Mr Smith and colleagues gave the misinformation campaign a rest.
Blog by Neil FrancisPosted on Tuesday 19th April 2016 at 2:00am
Lyle Shelton's bunkum tweet is broadcast on ABC's Q&A program
The Managing Director of the Australian Christian Lobby, Mr Lyle Shelton, is at it again.
Yesterday, he tweeted ABC's Q&A program as thousands of people do while it is on air. His tweet was broadcast live to air as shown above. What did he say as panelists were discussing assisted dying law reform?
"Sadly voluntary euthanasia quickly became involuntary euthanasia in Holland. #qanda" LyleShelton
Mr Shelton's claim is bunkum.
Confused language
Firstly, he's confused involuntary with non-voluntary euthanasia.
Involuntary euthanasia is the deliberate hastening of the death of an individual in contravention of the express wishes to the contrary of that individual. Nobody (except the Australian Christian Lobby in its confusion) is seriously suggesting that involuntary euthanasia happens in the Netherlands, even as a 'result' of the country's euthanasia law.
Non-voluntary euthanasia is the deliberate hastening of the death of an individual without an explicit request from that individual. Increased doses of analgesics and sedatives are administered to alleviate intractable symptoms at the end of life, as a result of discussion between doctors and the patient's family (the patient is not currently competent to participate in decisions). The drugs may hasten death and if this happens, life is shortened by hours, or less often, days. Despite claims by some assisted dying opponents that this is unique to the Netherlands, scientific research shows clearly that the practice occurs all over the world and is not 'caused' by voluntary euthanasia laws.
ACL staff sing from the same hymn book
Daniel Flynn, Victorian Director of the Australian Christian Lobby, made a similar claim in a formal submission (#694) to the Victorian Parliament's Inquiry into End Of Life Choices:
"There is sufficient evidence to suggest that involuntary euthanasia is frequent in jurisdictions in which euthanasia has been legalised." [p 4.]
Not a shred—let alone 'sufficient'—evidence was offered to back up this silly myth, though it's hardly surprising given that there isn't any.
What does the evidence actually show?
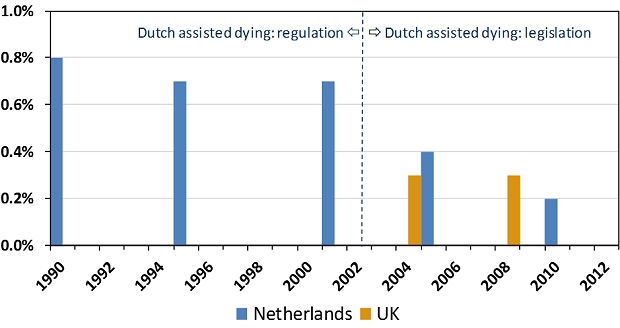
The scientific evidence is crystal clear and it is the opposite of Lyle Shelton and the Australian Christian Lobby's claim. Since around 1985 the Netherlands had permitted assisted dying by regulation: under agreement amongst relevant authorities. The rate of non-voluntary euthanasia remained relatively unchanged under this arrangement (Figure 1). In 2002 the Netherlands' euthanasia Act came into effect, replacing regulatory arrangements with a comprehensive set of legislative (i.e. statutory) requirements.
Figure 1: Netherlands and UK non-voluntary euthanasia rates
Since 2002, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen.1 The drop is statistically significant. The rate of non-voluntary euthanasia in the Netherlands is now around the same level as in the United Kingdom.2 The UK is generally accepted as the world's gold standard in palliative care practice and it does not have an assisted dying law.
Absolutely contrary to the claim of the Australian Christian Lobby's Lyle Shelton, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen. It's now similar to the rate in the UK, which has no assisted dying law.
ABC news standards
Since the ABC moved the Q&A program from its entertainment division to its news division there is a heighted obligation on the broadcaster to ensure that the show's content is reason- and evidence-based, and not merely a platform for anyone to promote silly misinformation in support of a perspective.
No doubt the ABC will rise suitably to the occasion of discouraging misinformation and ensuring that any is corrected.
We'll be watching the next episode of ABC Q&A closely to fact check anything Mr Shelton and others say about assisted dying law reform. Give us a bell if you spot anything you know or suspect is untrue.
---------------
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliative Medicine, vol. 23, no. 3, pp. 198-204.
The F filesPosted on Tuesday 22nd March 2016 at 12:00am
One of the articles wrongly claiming 650 Dutch babies euthanized
Opponents of assisted dying have fallen prey to misinformation contagion about the Dutch Groningen Protocol, claiming that 650 babies would be or are euthanized every year. The claim is comprehensively and evidentially false.
Starting in 2013 and increasing in shrillness in 2015, numerous opponents of assisted dying law reform—many of whom are connected to conservative (Christian) sources—published online articles making false claims about the Dutch Groningen Protocol, wrongly claiming that up to 650 babies could be, would be or actually are ‘euthanized,’ ‘killed’ or ‘murdered’ every year under the Protocol’s provisions.
A national Dutch Regulation (not statute) effective since late 2006 whose current name is so long that it remains convenient to use its old name, ‘Groningen Protocol,’ even though it has changed.
Permits, only as a last resort and with a number of strict conditions, the intentional ending of a newborn’s life when the newborn is in current (not merely anticipated) untreatable and unrelievable extremis.
Mandatory reporting of intentionally hastened deaths to a national Commission and the Board of Prosecutors General at The Hague.
Physician is not cleared until the case is deemed acceptable by the Commission and the Board and the Minister of Security and Justice.
The Regulation is entirely separate from and unrelated to the Dutch Euthanasia Act for competent adults.
Where did the '650 babies euthanized' claim come from?
In 2013 the Royal Dutch Medical Association (KNMG) published a media release that launched a major policy paper about end-of-life decisions for neonates. The media release stated that of the approximately 175,000 births in the Netherlands each year, around 650 newborns will die as a result of severe congenital defects.
Some of these babies die soon after birth, in the delivery room. Others die later in neonatal intensive care despite the best interventions attempting to keep them alive. Yet others die after futile treatment is withdrawn and palliative (comfort) care is administered to minimize suffering prior to death.
Only in a tiny minority of cases is there a medical intervention with an explicit intention to hasten the death of the newborn, who is in untreatable and unrelievable extremis.
Despite this clarity, opponents—mostly linked to conservative religious sources—jumped on the misinformation bandwagon and trumpeted that 650 babies either could be or would be or are actually ‘euthanized,’ ‘killed’ or ‘murdered’ every year in the Netherlands.
What's the actual evidence?
Neonatal euthanasia occurs around the world regardless of prohibition and is not caused by a protocol or regulation
For example, the rate in France, with no regulation, is much higher than the Netherlands.
Intentional hastening of neonatal death in the Netherlands is rare
Most neonatal deaths occur either quickly with no medical intervention, or intensive treatment proves futile and palliative (comfort) care is administered until death.
The (Groningen) Regulation has been further restricted since it was first formulated
It has not been 'relaxed' as claimed by some opponents.
The Regulation is separate from and completely unrelated to the Netherlands' Euthanasia Act
The Euthanasia Act is only for mentally competent adults (and 12-16 year olds with parental agreement).
Physicians do not receive black-letter law protection as they do under the Euthanasia Act
Reporting, investigation and acceptance requirements are even more rigorous than under the Euthanasia Act.
The rate of intention to hasten neonatal death has decreased since the Regulation came into effect
In eight years prior to Regulation there were twenty two reported cases, and only two in eight years since Regulation.
The rate of medical end-of-life decisions with an explicit intention to hasten death was 8–9% prior to Regulation, dropping to 1% after Regulation.
The use of neuromuscular blockers has decreased.
Physicians report improved communication with parents
Shared decision-making and better opportunities for parents to grieve the loss of their child.
There are clear explanations for the decrease in neonatal euthanasia in the Netherlands:
Physicians report they are fearful of prosecution under the Regulation, so they now more often administer palliative care not intended to hasten death.
A folate supplementation program for pregnant females has resulted in a substantial drop in the rate of spina bifida and related disorders.
An antenatal screening program at 20 weeks has resulted in a higher rate of pregnancy terminations for major congenital disorders.
In conclusion
Despite all these facts, in an epidemic of 'confirmation bias' that drove misinformation contagion, many anti-euthanasia commentators have published false claims about '650 babies euthanized' under the Dutch Groningen Protocol. I provide a forensic examination of the issue in the latest edition of the Journal of Assisted Dying.
This is not the first example of how opponents of assisted dying widely circulate information that is untrue (e.g. check out the Council of Europe Declaration 1859 case), and it won't be the last. However, for opponents of assisted dying to avoid egg on face, I'd recommend:
Neonatal deaths under Dutch Groningen Protocol very rare despite misinformation contagion
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 1, no. 1, pp. 7–19.
Abstract
The Groningen Protocol specifies criteria for the potential termination of life in severely ill newborns in extremis with untreatable and unrelievable conditions. In September 2006 the Netherlands formally adopted a Regulation incorporating the Protocol. Despite the Regulation’s development through extensive professional consultation, endorsement by the Dutch Paediatric Association, empirical data showing a decrease rather than increase in use, and research showing that neonatal euthanasia occurs around the world in the absence of regulation, the Dutch Regulation has sparked controversy. More recently it has been claimed that hundreds of babies a year are killed under its provisions. Forensic analysis reveals the claim to be comprehensively and evidentially false. Wide online dissemination of the claim by mostly religious sources demonstrates confirmation bias and misinformation contagion.
Francis, N 2016, 'Neonatal deaths under Dutch Groningen Protocol very rare despite misinformation contagion', Journal of Assisted Dying, vol. 1, no. 1, pp. 7-19.
Blog by Neil FrancisPosted on Saturday 2nd January 2016 at 12:35am
Dr William Toffler (left) acknowledges no slippery slope cause-and-effect evidence, with Drs Bentz and Stevens
A new scholarly journal focused on end-of-life ethics, decision-making and practice has just been launched: the Journal of Assisted Dying. In the first article, claims by Oregon lobby group Physicians for Compassionate Care (PCC), including Doctors Bill (William) Toffler and Ken Stevens (and others) are assessed against empirical evidence and found to be completely wrong, or highly misleading as a result of selective use of data.
The new scholarly journal, the Journal of Assisted Dying, is dedicated to careful and holistic analysis of evidence in regard to the various forms of assisted dying that are lawful in a number of jurisdictions around the world... and to practices in jurisdictions where assisted dying remains illegal.
In the first article of a series on Oregon, I examine claims and speculations made by various doctors (and others who quote them), that Oregon has the second-highest suicide rate in the USA (or is always in the top 10), that Oregon's Death With Dignity Act has resulted a massive increase in the state's general suicide rate, and other astonishing statements.
Of course, the empirical evidence from the Oregon Health Authority and from the USA Centers for Disease Control and Prevention does not support these statements and interpretations, and I analyse and critique the evidence.
Some of the claims are just plain factually and hugely wrong. Others are the result of failing to read their sources more carefully, misunderstanding what the data actually represents. Still further claims are made on the basis of selectively-chosen statements from government reports, while omitting statements that are contrary to, or provide alternative and well-researched explanations for Oregon's recently rising general suicide rate.
Drs Toffler and Stevens have even published some of their claims and speculations in the British Medical Journal.1 It goes to show that even good journals sometimes publish bunkum: their article was a letter to the editor rather than peer-reviewed research. Great care is required to sort real evidence from hype and opinion.
Ultimately, Dr Bill Toffler of PCC has acknowledged on video that there is no cause-and-effect evidence between Oregon's Death With Dignity Act and Oregon's suicide rate, an acknowledgement that went unchallenged by his two PCC colleagues present at the time, Dr Ken Stevens and Dr Chuck (Charles) Bentz. You can see Dr Toffler's statement here (at 10'50").
The Journal of Assisted Dying is an open-access journal, and you can read the full article here.
-----
1. Toffler, WL & Stevens, K 2015, 'Re: Assisted dying: law and practice around the world', BMJ, vol. 351, 19 Aug, p. h4481.
Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 1, no. 1, pp. 1–6.
Abstract
Background: Several physicians have speculated that Oregon’s general suicide rate is evidence of suicide contagion as a result of Oregon’s Death With Dignity Act (‘the Act’). Methods: Search and analysis of physician and related online sources of Oregon suicide contagion speculation; retrieval and analysis of cited Centers for Disease Control and Prevention (CDC) and other publications relied upon; analysis of authoritative, public Government mortality data for Oregon and other USA states. Results: Several physicians have speculated about Oregon suicide statistics in a manner that is not supported by the cited publications, or by public CDC mortality database data. The claims variously (a) misrepresent key data in the publications, (b) omit information in the publications that is at variance with suicide contagion speculation, and (c) overlook other significant information at variance with speculation. The physicians have previously acknowledged inability to prove perceived “slippery slope” effects of the Act. Other opponents of the Act have republished the physicians’ erroneous information. Conclusions: Evidence advanced by several physicians to speculate that Oregon’s Death With Dignity Act causes suicide contagion in Oregon is variously false, misleading or highly selective—omitting key facts—and has arisen even though the physicians acknowledge they have no proof of ‘slippery slope’ effects.
Article keywords
suicide contagion, copycat suicide, Werther effect, slippery slope, misinformation, Oregon, Dr William Toffler, Dr Kenneth Stevens, Physicians for Compassionate Care
Full PDF
Download the full PDF: (390Kb)
Citation
Francis, N 2016, 'Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon', Journal of Assisted Dying, vol. 1, no. 1, pp. 1-6.
Blog by Neil FrancisPosted on Wednesday 25th November 2015 at 8:00pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
On Wednesday 19th November 2015, the Catholic Church appeared before the Victorian Parliament's Legal and Social Issues Committee. Monsignor Anthony Ireland, the Episcopal Vicar for Health, Aged and Disability Care, and Father Anthony Kerin, Episcopal Vicar for Life, Marriage and Family gave evidence about end-of-life decision making. They made a factually wrong allegation about Oregon during their testimony.
Anthony Ireland spoke first, making it clear that they were appearing before the Committee with delegated authority from the Catholic Archbishop of Melbourne (Denis Hart) and with the endorsement of the Victorian Catholic Bishops. He emphasised that "the Catholic Archdiocese of Melbourne does not come to this Committee with fanciful or frivolous arguments."
During question time. Committee Chair Edward O'Donohue asked the Vicars if they had any evidence from lawful jurisdictions to back up their claim that legalising assisted dying would result in a significant reduction in medical research. The Vicars flailed about with vague hypotheticals, but no evidence.
Committee Deputy Chair Nina Springle remarked that some of their testimony was inconsistent with direct evidence from lawful jurisdictions and invited them to reflect on the contradictions. To this, Anthony Kerin stated:
"We know, for example, since Oregon legislated, that the standard suicide rate has increased remarkably and alarmingly. It's not yet the largest rate in the US, but it's getting there, when Oregon had a very, very low suicide rate prior to that."
Let's not mince words: the allegation is comprehensively false. In fact it's three false statements all wrapped up into one.
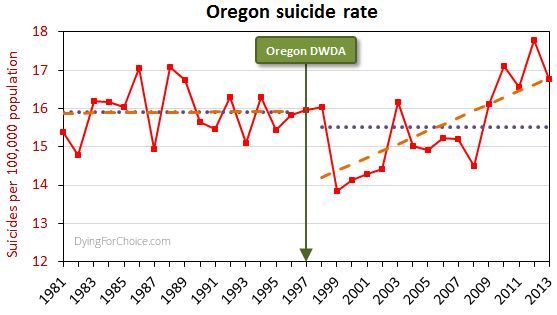
The USA government's CDC mortaility database provides solid empirical data. Here's Oregon's longitudinal suicide rate statistics, including sixteen years before its Death With Dignity Act (DWDA), and sixteen years after.
Here are the pertinent facts about Oregon's general suicide rate:
The average for the 16 years after the DWDA is lower than, but not statistically different from, the 16 years prior to the Act.
There was a massive drop in the suicide rate two years after the DWDA came into effect, and the rate has risen only from there.
The rise from 2000 onwards is repeated in the majority of USA states and in the national average. The trend increase in Oregon is not statistically different from the national trend increase.
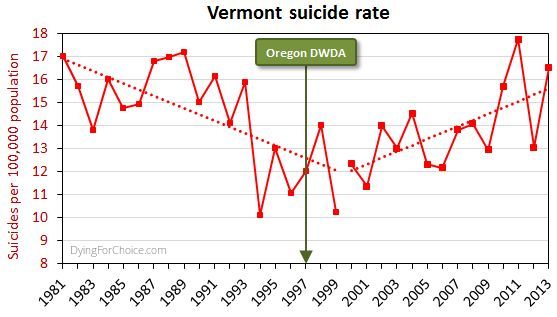
By way of comparison, here's Vermont's suicide rate for the same period.
Now, Vermont didn't have an assisted dying law until 2013, and no assisted deaths occurred under the law in that year, so the suicide rate cannot have been affected by an assisted dying law. Yet the picture is similar to Oregon's.
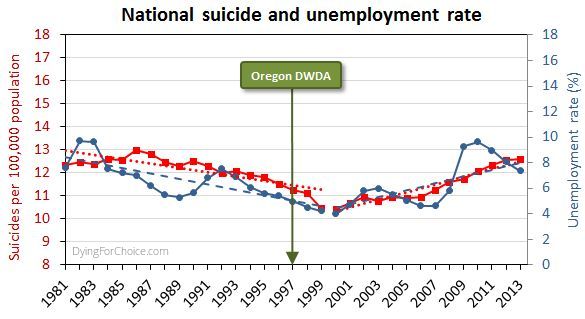
Here's the USA national suicide rate for the same period, with the unemployment rate added.
There are numerous and complex reasons for suicide and for changes in the rate, but a key one in this USA case is unemployment, which after falling in the 1990s rose abruptly from 2000 onwards.
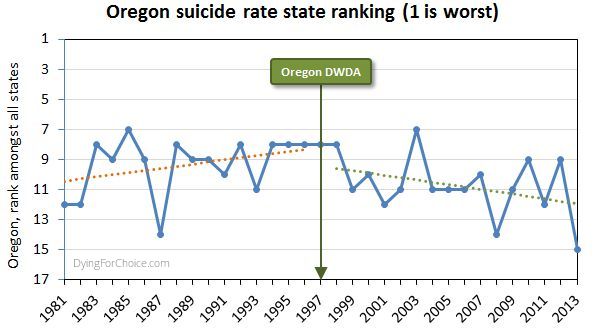
Has Oregon's suicide rate been worsening relative to other USA states, though? The state annual suicide rankings are informative.
Prior to the DWDA, the trend in Oregon's suicide ranking among all USA states was deteriorating (where ranking number one is the highest suicide rate). Since the Act came into effect, the trend is improving. The difference in trends is statistically significant. In the sixteen years since the Act came into effect, Oregon has appeared in the "top ten" six times, compared with twelve times in the 16 years prior to the Act.
So, let's examine the three elements of the Catholic Church's statement:
1. "Since Oregon legislated, the standard suicide rate has increased remarkably and alarmingly"
This statement is false by omission. It is critically relevant to mention that Oregon's suicide rate dropped massively two years after the DWDA came into effect. Only after 2000 did it begin to rise—like most states and nationally—and in response to a rising unemployment rate.
2. "Oregon had a very, very low suicide rate prior to that [the DWDA]"
This statement is completely false. Oregon's mean rate suicide for 16 years after the act is not significantly different from the mean for 16 years prior to the Act. Indeed, government data back to 1968 shows Oregon's general suicide rate has always been high and never "low", let alone "very, very low".
3. It's not yet the largest rate in the US, but it's getting there"
This statement is completely false. Oregon's suicide ranking amongst USA states was worsening prior to the DWDA, but has been improving since.
It's very disappointing indeed that the Catholic Archdiocese of Melbourne would offer such profoundly false testimony to a legislative committee making inquiries on behalf of the people of Victoria. The offense is all the more grevious because of the unequivocal manner in which the statement was made, and that the witnesses specifically stated they did not bring any fanciful or frivolous arguments to the Committee.
It's time to comprehensively stamp out false information about assisted dying, no matter how fervently it might be believed by its proponents. Watch this space: there's plenty more to come!
Blog by Neil FrancisPosted on Sunday 15th November 2015 at 2:38am
ABC TV's Q&A panel discusses assisted dying law reform on 9th Nov 2015
In a recent opinion piece in the ABC’s Religion and Ethics section, Bernadette Tobin1 rails against assisted dying, commencing with the criticism that the ABC’s Q&A discussion on the subject this week “lacked precision.” But Tobin’s opinion piece itself commits exactly this offence, as I explain.
For the sake of brevity I’ll only quickly mention that Tobin’s piece also fails on the score of accuracy. For example, she wrongly asserts that “euthanasia” means a doctor administering lethal medication to a patient. It doesn’t. “Euthanasia” simply means “good death”: nothing more and nothing less, regardless of how it occurs. Tobin also asserts that voluntary euthanasia in lawful jurisdictions has caused non-voluntary euthanasia to develop. This is the polar opposite of published empirical research evidence.
But back to precision. Tobin employs two imprecise and deeply flawed arguments in her objection to assisted dying. She variously rolls them in together, so let’s unpack what they are: (A) the “it’s only fair” slippery slope, and (B) “it’s OK if you don’t mean it”.
A: The “It’s only fair” slippery slope
Tobin directly links assisted dying for the terminally ill to “anyone who is in pain, discomfort, constipated, incontinent, depressed, anxious and so on” by way of potential “benefit”. She conjectures that increasing the restrictions to who may qualify, and the process of qualification, would then be “unfair” to these others. She then goes on to extend the argument to those lacking in decisional capacity such as infants and those with Alzheimer’s. Surely, she says, “it would be ‘unfair’ to deny these people the ‘benefit’ that we will make available to those who are able to request it?”
Slippery slope indeed. And it’s wrong. Let me illustrate how, using a topic familiar in political debate over recent years: same-sex marriage.
Opponents of same-sex marriage law reform, when using arguments of the kind Tobin offers (as they often do), say that we can’t allow two men to marry, or two women to marry, because then we would have to allow three or more people to marry. Further down the slippery slope, we would have to allow people to marry animals. Don’t laugh: such things have been argued.
Next—given that under the Corporations Act 2001 (Cth), companies, owners’ corporations and incorporated associations are at law ‘persons’, and now that persons may marry—it would be “unfair” (note that I’ve used imprecision quotation marks around the word as Tobin does) to disallow people from marrying companies and companies from marrying each other.
Finally, using Tobin’s own line of argument, it would be “unfair” to deny infants and those with Alzheimer’s being married off for the alleged “benefit” (those quotation marks again) that everyone else is enjoying, so we must as an unavoidable consequence of the first step of allowing same-sex marriage, allow arranged marriages for babies and those with advanced dementia.
By now it’s easy to spot two terminal flaws in Tobin’s argument.
Firstly, the use of just one criterion (“fairness”—which she leaves imprecisely undefined) as the sole basis for decision making about this legislative reform is indefensible. What about other critical factors such as well-informed, rational, decisional capacity, judging and weighing what a “benefit” is, in the face of intolerable and unrelievable suffering, consistent with one’s own values and beliefs, who may decide, and the right not to participate?
Secondly, any slippery slope’s purported summit (from which changes are argued only to slip downwards) is deeply rooted in the normativity of the present. We are used to marriage being between a man and a woman. In our relative comfort we accept it as ‘normal,’ ‘good’ and the ‘right thing’.
In decision-making scholarship this normativity is known as “anchoring”. Like an anchor around which a boat will swing according to the wind and tide, we take the pivot point (the anchor of the now), as the natural starting point for future decisions, comparing changes only to the present state of affairs.
But it isn’t a valid anchor, and assuming that it is seriously biases our thinking. We need cast our anchor back just one mooring from the current point to see how the anchor tints our decision-making spectacles:
“We can’t allow a man and a woman to marry, because then it would be unfair to not allow two men to marry, or two women to marry, and then…”
Clearly, it is imperative that we outlaw marriage altogether.
The upshot of this slippery slope, when followed properly to its own logical conclusions, is that we must deny all rights because we can confect a slippery slope into a hypothetical moral abyss for any right.
B: It’s OK if you don’t mean it
Tobin further argues that relieving distressing symptoms “is good palliative care, even when that relief happens to hasten death.”
She doesn’t name it explicitly, but this is the doctrine of double effect, an argument first crafted in the thirteenth century by Catholic priest Thomas Aquinas. The doctrine suggests that a bad consequence of an action is justifiable if the agent did not intend the bad effect, if the intended good effect outweighs the bad effect, and if the agent applies diligence in attempting to minimise the bad effect. Notice that the doctrine speaks directly about the intentions of the agent and is silent on the views of the person upon whom the agent might act.
Tobin rails against a doctor intentionally administering a lethal dose to a patient (regardless of whether it is the dying patient’s most fervent wish) and slams the expressions “dying with dignity” and “aid in dying” as “fudges”.
Yet the doctrine of double effect, for which she argues in support, is itself a fudge because it says:
“It’s OK to for a doctor to decide to and actually kill their patient (after all, they hastened the patient’s death), as long as they don’t mean to, and they mean well.”
What kind of standard is the secret stuff that goes on inside a doctor’s head without reference of any kind to the patient’s own views and desires, when compared to a fully informed, documented and tested request from the patient?
It’s no wonder that many scholars (as do I) consider the doctrine of double effect problematic.
--
Bernadette Tobin is the Director of the Plunkett Centre for Ethics, a joint initiative of St Vincent’s Hospital, Sydney, and Australian Catholic University (ACU). According to ACU, a core mission of the Centre is to “bring a Catholic perspective to all its endeavours”.2
It’s unsurprising then that I detected neither broad thrust nor any detail of Tobin’s ABC opinion piece that deviated from the views of the Vatican. So be it.
There are many points on which Tobin and I agree, such as the potential benefits of palliative care for the dying. I argue, though, that basic scrutiny of the proffered 'principles' reveal them as deeply flawed and unpersuasive.