Blog by Neil FrancisPosted on Thursday 17th September 2015 at 6:06am
On 16th September 2015, the Victorian Director of the Australian Christian Lobby (ACL), Dan Flynn, appeared as a witness to the Victorian Parliament’s end of life choices inquiry being conducted by the Legal and Social Issues Committee. He made a number of mistaken statements, but what was most worrisome was the revelation of the ACL’s real agenda: to wind back patient rights more than a quarter century.
In his opening address, Mr Flynn opined that assisted dying was 'not supported' by a 'broad base' of Victorian Christians (not just the ACL). This belief is diametrically at odds with clear and repeated evidence from multiple sources.
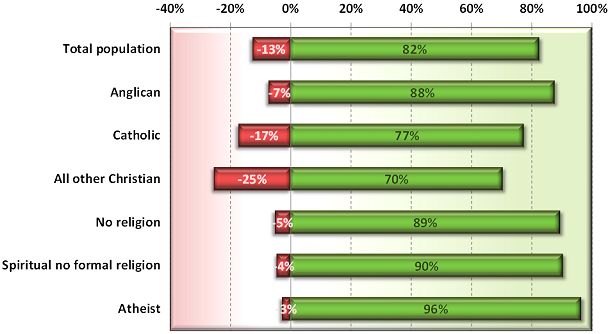
In 2012, I reported on a Newspoll study into Australian attitudes towards assisted dying. Not only did a whopping majority of citizens support assisted dying, but so did a great majority of Anglicans, Catholics and other Christians (Francis 2012).
Newspoll 2012: Australian attitudes to assisted dying law reform by religion (green=support, red=oppose)
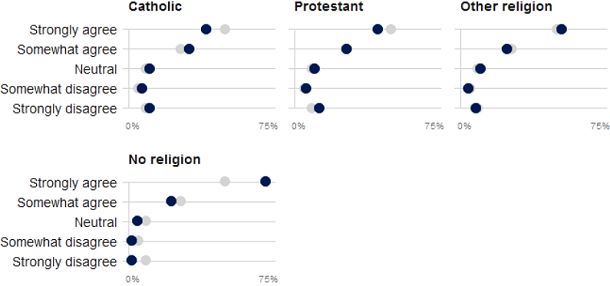
These national results are reflected by a sample of over 60,000 Victorians through the VoteCompass system during the 2014 Victorian election (Stayner 2014). It confirms a substantial majority of Catholics, Protestants, other religious and non-religious Victorians support assisted dying law reform.
VoteCompass 2014: Victorian attitudes to assisted dying law reform by religion (grey=population average)
Out of date
Mr Flynn then referred to a Tasmanian Parliament’s inquiry into assisted dying which rejected law reform. However, the inquiry to which he refers was held in 1998, when Oregon’s Death With Dignity Act had barely been established, the Northern Territory’s Rights of the Terminally Ill Act had been extinguished within just eight months of coming into operation, and the Dutch, Belgian, Luxembourg, Washington and other legislation and judgements did not yet exist.
So, the Tasmanian Parliament’s rejection came from a position of a then general lack of information. The Oregon law has been in effect since 1997, the Netherlands and Belgium since 2002, Washington since 2008, Luxembourg since 2009, and so on. There is now plenty of evidence that assisted dying law reform doesn’t cause slippery slopes that opponents love to theorise about.
Wrong about ‘United Nations’
Mr Flynn then said that the United Nations had in 2012 expressed concern about a ‘lax attitude’ towards euthanasia in Europe, specifically mentioning the Netherlands and Belgium. This is completely untrue. Because it’s easy to make a simple blooper during a presentation, we’ll put aside the fact that he meant to refer to a completely different organisation: the Council of Europe.
We know this because he read directly from Council of Europe declaration 1859 (Council of Europe Parliamentary Assembly 2012). His ACL submission (Australian Christian Lobby 2015) reports (as he read out) exactly one sentence of the declaration, with his added emphasis, as:
"Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited."
But presented in this manner the statement is quite misleading. As I explain in a forensic analysis of the misinformation campaign about this resolution (Francis 2015), the resolution was utterly clear about its intent: it was not about euthanasia (it explicitly said so), but rather about advance care planning. What the resolution spoke against (in the one sentence conveyed above) is non-voluntary euthanasia, not voluntary euthanasia. Both sides of the assisted dying debate agree that non-voluntary euthanasia (one person deciding for a hastened death on behalf of another) is not acceptable. It is not contentious.
In no way did the Council of Europe's resolution critique voluntary euthanasia or comment on any jurisdiction in which it is legal. And, the United Nations source to which the ACL submission refers was released in 2001, fourteen years ago and at the time of the Netherlands' Euthanasia Act was before the Dutch Parliament. With then limited information about how such laws work in practice, it expressed concern about the upcoming Act.
Wrong about Belgium’s law and practice
Mr Flynn referred vaguely to two cases of euthanasia in Belgium in which persons who requested and received euthanasia were not experiencing intolerable pain, which Mr Flynn asserted was a required safeguard in Belgium’s euthanasia Act. This was another supposed example of transgression of safeguards. Wrong again.
While the Belgian Euthanasia Act is officially published only in Dutch and French, a robust English translation has been prepared under the supervision of Professor Herman Nys of the Centre for Biomedical Ethics and Law at the Catholic University of Leuven (see Parliament of Belgium 2002). The word ‘pain’ does not appear in the Act… at all. What does the Act have to say about the legislature’s intent on who may qualify? The relevant clause in Section 1 says:
— "the patient is in a medically futile condition of constant and unbearable physical or mental suffering that can not be alleviated, resulting from a serious and incurable disorder caused by illness or accident."
It’s abundantly clear: mental suffering from an illness or accident qualifies as much as physical suffering, and the suffering does not need to be ‘pain’ as Mr Flynn mistakenly asserted to the Parliamentary Committee.
Mr Flynn also stated that there are mobile end-of-life units in Belgium. There aren’t. (But there are in the Netherlands, and they must follow precisely all the same requirements as anyone else. They operate to provide choice to patients whose regular or reachable doctors disagree with assisted dying and therefore decline to evaluate whether the patient may qualify under the Act.)
Confused about Advance Care Directives
In further testimony, Mr Flynn opined that the degree to which a doctor should be allowed to override a patient’s Advance Care Directive (ACD) is in part influenced by whether the doctor can speak with the patient.
But if the patient can currently speak and participate in decision-making, the advance care directive doesn’t apply: it is mute and of no effect. An ACD only applies when the patient cannot currently participate in their own decision making. That’s (only) what it’s for.
Winding rights back more than a quarter century
But the most worrying aspect Mr Flynn’s testimony was the revelation of ACL’s opposition to the right to refuse unwanted medical treatment.
The Medical Treatment Act 1998 (Vic) has enshrined for now more than twenty five years a patient’s right to refuse any unwanted medical treatments. In 2003 the Supreme Court of Victoria determined that artificial nutrition and hydration (i.e. via tubes) is medical treatment and can therefore be refused under the Act.
But Mr Flynn repeatedly argued that withholding or withdrawing artificial nutrition and hydration, if the patient’s body could ‘absorb’ them, could amount to physician-assisted suicide, and that doctors must be allowed to override refusals. On the matter of patient autonomy, he said that some autonomy rests "with the patients, but a lot of the autonomy in fact is with the doctor”.
When asked if a Jehovah's Witness who refuses a life-saving and simple blood transfusion ought to be allowed to do so, he conceded that they should be entitled to, but that such a case was a “bit of an outlier”. He didn’t explain on what moral grounds one person could refuse a simple procedure to save their life, but another person mustn’t be allowed to even if the likelihood of saving life was doubtful.
So, the ACL’s real agenda is revealed: it recommends winding back the legislative clock more than a quarter century so as to force patients to endure some medical interventions that they don’t want and firmly refuse, if the doctor wishes to proceed.
No wonder the Committee repeatedly questioned Mr Flynn to ensure they had heard and understood his testimony correctly. In conclusion, Committee Chair Edward O’Donohue observed that Mr Flynn’s evidence was “quite surprising” and “quite contrary” to wide evidence already given.
And it’s no wonder that Theo Mackaay, General Secretary of the Victorian Council of Churches—a group of 30 member churches representing mainstream Christianity—criticised the ACL as “fundamentally conservative” and expressed “deep concern that media portrayal of statements from an established and narrow focused lobby group is presented as being representative of the entire Christian community” (Uniting Church in Australia 2011).
-----
References
Australian Christian Lobby 2015, Submission to the Legal and Social Issues Committee on the Inquiry inito End of Life Choices, Parliament of Victoria, Melbourne, pp. 1-17.
Council of Europe Parliamentary Assembly 2012, Resolution 1859 (2012): Protecting human rights and dignity by taking into account previously expressed wishes of patients, Europe, 25 Jan, pp. 2.
Francis, N 2012, Australian public desire for legalisation of assisted dying in restricted circumstances, YourLastRight.com, Melbourne, pp. 11.
Parliament of Belgium 2002, 'The Belgian Act on Euthanasia of May 28th 2002 (unofficial English translation)', Ethical Perspectives, vol. 9, no. 2-3, pp. 182-188.
Uniting Church in Australia 2011, Australian Christian Lobby does not represent all Australian Christians, nor all Christian viewpoints, 8 Dec, Media Room, viewed 11 Dec 2011, <http://blogs.victas.uca.org.au/mediaroom/?p=971>.
Blog by Neil FrancisPosted on Thursday 23rd July 2015 at 1:22am
The Victorian Premier doesn't support assisted dying law reform - at this stage.
Victorian Premier Daniel Andrews reports that he doesn’t support voluntary euthanasia “at this stage” (The Age, 21 Jun 2015), and that his objections are not based on his Catholic faith. I think it is fair to take him at his word given his historical record in facilitating conversation and reform around values-based issues such as abortion. But his current thinking on assisted dying is indefensible as I explain.
We know from repeated Newspoll Australia studies that amongst the millions of Victorians who want the State to respect their wish to make their own choices at the end of life, three out of four Australian Catholics are in favour of legalised assisted dying—at odds with the ‘traditional’ Catholic stance. Mr Andrews, like a majority of Catholic Australians, may simply not agree with the Vatican line on assisted dying choice, as they don't on a range of matters.
Mr Andrews says that his current objections instead revolve around ‘safeguard’ and ‘balance’ issues in a context of finite healthcare resources.
The Medical Treatment Act 1988 confers the right to Victorian patients to refuse any medical treatment. The right applies even if the treatment is life-saving, for example a simple blood transfusion. The Act contains no ‘safeguards’, as the Premier refers to them:
The patient is not required to give any reason;
The doctor is not required to inform the patient of their condition or likely consequences of any treatment or its refusal;
The doctor is not required to consider or assess the patient’s mental capacity to decide including depression;
The doctor is not required to recommend a palliative consult (if relevant);
The doctor is not required to consult any colleagues for a further opinion about the patient’s illness or mental capacity;
There is no obligation on the patient to consider their decision again after a short time;
While there is a standard form 'Refusal of Medical Treatment' document that can be signed to provide documentary evidence of the refusal, it is not mandatory;
There is no mandated path of reporting or review.
Indeed, a doctor who goes on to administer medical interventions to the patient who has refused them is guilty of the offence of ‘medical trespass’ and can be prosecuted.
Further, it is quite legal for a patient to decide to die by voluntary refusal of food and fluids, an option suggested as appropriate by Dr Bill Sylvester in an IQ2 debate at Melbourne Town Hall in November 2012, to a hostile reaction from the audience. Some doctors provide respite care to patients choosing this path. however, like refusal of medical treatment, there are no legislated safeguards.
On the basis of these two kinds of end-of-life decision making that have been lawful for at least a quarter century in Victoria, and which have no legislated safeguards, what evidence do we have of the so-called ‘slippery slope’ of resource-strapped healthcare providers or greedy relatives persuading the sick to choose a path to die earlier rather than later?
Both Victoria Police and the former Minister for Health, the Hon. David Davis, have advised that there are no known prosecutions under the provisions of the Medical Treatment Act 1988 for such inappropriate persuasion.
So, in Victoria we have the experience of two forms of decision-making whose direct and foreseeable consequence is death, with no mandated safeguards and within 'finite healthcare resources' (which Mr Andrews refers to as his reason), not resulting in prosecutions for persuasion to 'choose' death.
If Mr Andrews’ argument is that terminally ill Victorians ought to be denied the right to choose assisted dying because of supposed slippery slopes of persuasion, that argument would exactly and equally apply to the refusal of life-saving medical treatment and to the refusal of food and fluids.
Surely his Government is not suggesting that the existing rights be rescinded: that patients be forced to receive any and all life-saving and life-prolonging treatment in order to avoid a 'persuasion' bogeyman who doesn’t exist?
The Premier's stance is even less defensible in the light of proposed assisted dying legislation which includes a suite of checks and balances that are absent from existing rights.
Some dying individuals, reflecting upon their circumstances and deeply-held values and beliefs, determine that alighting from the train of terminal illness one or two stops before the terminus is a vastly better option than being forced to endure the train ride until the very end. We compound their indignities by saying it’s OK to decide to starve yourself to death (and we might even provide support along the way), but not OK to decide to die peacefully surrounded by loved ones at a predetermined time.
It is commendable that the Legislative Council has resolved to investigate the issue of end-of-life decisions, and whose final report will better inform the Premier and all Parliamentarians. Submissions to the Committee are open until Monday 31st August.
The Hon. Bob Such's Ending Life With Dignity Bill 2013, before the South Australian Parliament, contains a strong compliment of safeguards, as Neil Francis explains in this video. The refusal of life-saving treatment, to which Australians are entitled but with the same direct and foreseeable consequence as doctor-assisted dying requests, have practically none of these safeguards, yet there has been NO avalanche of inappropriate persuasion to refuse life-saving medical treatment, as the so-called "slippery slope" hypothesis would have us believe.
This is the third of three videos sent to South Australian MPs in 2013.
VideoPosted on Saturday 21st September 2013 at 5:45pm
Opponents of assisted dying law reform often invoke fictional slippery slopes as objections to law reform. In this video, Neil Francis gives three examples of supposed slippery slopes argued by opponents, explains why they are fictional, and shares the perspectives of several recognised experts from the USA state of Oregon about their Death With Dignity law which has been in effect since 1997. Three long-time Oregonian Death With Dignity Act opponents also admit there's no cause-and-effect relationship established between law reform and supposed slippery slopes.
This is the second of three videos sent to South Australian MPs in 2013.