To use religion—or the claimed tenets of a particular version of a particular religion—to argue that all others should adhere to its values and abide by its rules of conduct.
Blog by Neil FrancisPosted on Sunday 6th August 2017 at 3:36am
Victorian MP Daniel Mulino's minority report contains multiple serious errors and misinformation.
Last year, the Victorian Parliament's Legal and Social Issues Committee concluded an extensive investigation into end of life choices, publishing a report of over 400 pages recommending improvements to palliative care and for assisted dying. Catholic-backed Shop, Distributive and Allied Employees' Association (‘shoppies’ union) Labor member of the Victorian Parliament Mr Daniel Mulino furnished his own minority report, opposing the majority recommendation for assisted dying law reform. That’s entirely his right. However, his report contains multiple, serious cases of misinformation. He must withdraw his report.
Daniel Mulino, Labor parliamentary member for the Victorian Region of Eastern Victoria,1 and a member of the Catholic-backed ‘shoppies’ union,2 was a member of the Legal and Social Issues Committee that thoroughly investigated end of life decision making and produced a 400+ page report in 2016 making recommendations for law reform and regulation.
Mr Mulino furnished a “minority report” as an addendum to the main report in order to oppose the Committee’s recommendation that assisted dying be legalised.3
Promoted by Catholics to Catholics
Mr Paul Russell, South Australian publisher of the Catholic anti-euthanasia website ‘HOPE,’§ says this of Mr Mulino’s minority report in the Catholic lawyer association’s blog:4
“Daniel Mulino MLC's analysis should be read first, before the Majority Report. It forms not only a sound academic and rigorous approach but also, by implication, is damning of the narrow, outcome focus of the Majority Report.”
How sweet of Mr Russell to so generously plug Mr Mulino’s report. But, in gushing about the ‘sound academic and rigorous approach’ he claims to be in it, shows that he doesn't understand what constitutes proper and sound evidence, and that he's easily impressed by charts and lots of ‘literature’ citations.
Numerous fundamental faults
The reality is very different.
Rather than bore you with a mind-numbing blow-by-blow dissertation on the numerous fundamental faults in Mr Mulino’s report, I’ll demonstrate how the report cherry-picks, misquotes and misunderstands its way through the evidence, via four revealing examples.
Example 1. Cherry-picking ‘helpful’ data
Mr Mulino’s minority report illustrates the rise in number of assisted deaths in the Netherlands and Belgium, and produces some statistics (Figures 1 & 2 are directly from his minority report).
Figures 1 and 2 (of Mr Mulino’s minority report): Assisted deaths in Belgium and the Netherlands
Note that Belgian data is for the years 2003–15, but the Netherlands only for the years 2008–15. That’s odd, because the euthanasia Acts for both countries came into effect in 2002, and so 2003 was the first full year for both.
Mr Mulino doesn’t point out that his report treats the two countries differentially, and provides no explanation as to why. We might notice, however, that the dicrepancy has the consequence of making his claims look 'better.'
Using Mr Mulino’s presentation style, Figure 3 illustrates all the relevant data for the Netherlands.
Figure 3: The full Netherlands data Source: Official Euthanasia Commission reports
As you can see, there is a virtual flatline between 2003 and 2007. Indeed, there is even a tiny drop in numbers between 2005–06. This is an inconvenient truth to Mr Mulino’s thesis that there has been a consistent massive rise in numbers. It also substantially reduces the compound annual growth rate he wrongly quotes for just 2008–15.
He’s also cherry-picked only raw data. In fact, the only valid way to compare year to year, and jurisdiction to jurisdiction, is to use the rate for each year: that is, the number of assisted deaths as a proportion of total deaths in the same year and jurisdiction, so that you’re comparing apples with apples. It's necessary because the total deaths count goes down and (mostly) up a bit each year. The official government statistics for total deaths by year for both countries are readily available online, so there’s no excuse for not using them.
When you calculate the rates, you get validly-comparable results, as I illustrate in Figure 4.
Figure 4: Rate of assisted dying as a percent off all deaths in the Netherlands and Belgium 2003–2015 Sources: Official government statistics; Euthanasia Commission reports
As I explain in my detailed research whitepaper on Benelux assisted dying,5 these are sigmoid (stretched-S) shaped curves which are typical of human behaviour change. And there is a drop in the rate in both countries in 2015, which Mr Mulino doesn’t report.
My Benelux whitepaper also reports the data from Luxembourg (Figure 5), which Mr Mulino fails to mention, even though it has legislation, since 2009, almost identical to the Netherlands and Belgium, and the Luxembourg government's data is freely available online.
Figure 5: Rate of assisted dying in the three lawful Benelux countries Sources: Official government statistics; Euthanasia Commission reports
Luxembourg’s data (yellow in Figure 5; no data available yet for 2015), is also an inconvenient truth to the case Mr Mulino attempts to prosecute. There’s no substantial rise.
Example 2. Comparing apples with oranges: mis-matching data
Mr Mulino again fails to compare apples with apples. Take, for example, his vocal claim that the annual total death counts for the Netherlands decreased at the same time as the total counts for assisted dying increased.
When you look at the data he’s used (the citation for the negative total deaths trend he quotes in his Table 2), you find that he’s used total death data for 2000–10, which is falling, while his assisted dying data is for 2008–15, which is rising.
This just isn’t on: it’s completely invalid to compare data like this from one period with data from another period to claim or imply a causal relationship. Of what possible relevance is the total death data for 2000–02, while his total deaths data for 2011–15 is missing? I illustrate the full story in Figure 6.
Figure 6: Netherlands total and assisted deaths for different periods Sources: Official government statistics; Euthanasia Commission reports
The solid blue and orange lines are data Mr Mulino used and reported, and their dotted ends are data that he omitted. It’s easy to see that the total deaths data his report inappropriately relies upon has a negative (downwards) slope (left-hand blue dashes), while the matching total deaths data he should have used has a positive (upwards) slope (right-hand blue dashes). Valid comparison gives lie to his claim.
Example 3. White is the new black: Misquoting the opposite
Mr Mulino’s report also argues that there’s ample evidence that a significant proportion of people with depression are gaining access to assisted dying:
“Ganzini et al, in a broad ranging review of instances of assisted dying in Oregon, found that twenty percent of the patients had symptoms of depression.” [Italics mine]
This assertion is nonchalantly plucked from the review6 without reading it properly, seemingly to support his thesis. In fact, the source does the exact opposite. Figure 7 is an image of the Abstract, where it says in large print, right up front:
“Twenty percent of the patients had symptoms of depression; none of these patients received a prescription for a lethal medication.” [Emphasis is mine]
Figure 7: The paper Abstract articulates exactly the opposite of Mr Mulino’s claim Source: Ganzini et al 20006
Had Mr Mulino bothered to read either the abstract or the methodology of this study properly, he would have realised that the doctor sample was of those eligible to prescribe under Oregon’s Death With Dignity Act, not just those who had, and that none of the study's patients who were assessed with possible depression had accessed an assisted death.
It's not like the information was hard to find — his report cites literally half a sentence to support his claim, when the full sentence says the opposite.
Example 4. Any port in a storm: Cherry-picking, misunderstanding and misrepresenting out-of-date data
In attempting to establish a 'slippery slope' from voluntary, to non-voluntary euthanasia (NVE) — a practice where doctors may hasten death (e.g. by administering increasing doses of opioids) when the patient hasn’t explicitly requested it — Mr Mulino states in his minority report:
“Two countries with the highest rates of this type of end-of-life (Belgium at 1.5% and the Netherlands at 0.60%) allowed the practice of euthanasia and assisted dying.”
Oh dear, Mr Mulino's report cherry-picks again. Just look at his source.7 The study, published in 2003, contains Table 2, with the relevant data in it (Figure 8).
Figure 8: Table 2 from the 2003 study Mr Mulino cites Source: van der Heide et al 20037
There are no fewer than five major offences Mr Mulino commits here.
Firstly, look at the table. I’ve highlighted the line in yellow from which Mr Mulino draws his figures of 1.5% for Belgium and 0.60% for the Netherlands. You can immediately and easily see that Denmark’s rate of 0.67% is higher than the Netherlands' of 0.60%.
So, Mr Mulino’s statement mentioning only Belgium and the Netherlands with “highest NVE rates” is misleading. He failed to either report or explain why Denmark’s rate is higher than the Netherlands, while Denmark doesn’t have an assisted dying law; the opposite of his thesis.
Secondly, he also fails to mention Switzerland’s NVE rate of 0.42%, or to explain that it’s lower than the Netherlands and Belgium. That’s highly relevant, because Switzerland has the world’s oldest assisted dying law — in effect since 1942 — and its statute contains none of the safeguards in the Belgian and Dutch Acts. This too is at odds with Mr Mulino’s thesis.
Thirdly, if Mr Mulino had read the study properly instead of just cherry-picking convenient figures from it, he would have noticed in the methodology section that the fieldwork (doctors filling in questionnaires) was completed in 2001 and early 2002, that is, before either the Netherlands or Belgian Acts came into effect later in 2002 (the Netherlands in April and Belgium in September).
Thus, the Dutch and Belgian data points Mr Mulino advances as ‘evidence’ of an NVE ‘slippery slope’ from legislated assisted dying have nothing whatever to do with assisted deaths under their Euthanasia Acts, because neither Act existed at the time the study was conducted.
Fourthly, he is resorting here to a single point-in-time study, which has little to no scientific power to establish ‘causation’. To really establish causation, as a minimum you have to assess longitudinal data, which I show in Figure 9. It demonstrates the precise opposite of Mr Mulino's ‘slippery slope’ thesis that voluntary euthanasia causes NVE, which if true would lead to a significant increase in the NVE rate in both countries after statutory legalisation.
Figure 9: Longitudinal NVE rates in the Netherlands, Belgium and the UK Sources: Netherlands8; Belgium9; UK10
Both the Dutch and Belgian NVE rates have dropped with high statistical significance since their euthanasia Acts came into effect. Indeed, the NVE rate in the Netherlands is now similar to the rate in the UK, which is acknowledged as the world’s gold standard in palliative care and which hasnever had an assisted dying law. This is consistent with assisted dying law reform shining a bright light on all end of life practices.
It’s not like he simply didn’t know
Fifthly, it’s particularly disappointing that Mr Mulino’s report only cherry-picked outdated data in an attempt to ‘prove’ his case when I had already directly furnished the current relevant evidence to his Committee as a properly-researched formal submission: Figure 9 above is Figure 19 in my submission, and I provided the peer-reviewed research citations for the data.11
Not only that, but the official transcript of my appearance as an expert witness before the parliamentary Committee confirms that Mr Mulino specifically quizzed me on that Figure 19 and I pointed out the sources of its data:12
“Mr MULINO — Figure 19, for example.
Mr FRANCIS — The reference should be in the text. The last sentence on the previous page gives you the citations for that data.
Mr MULINO — Okay.”
Even further, when fellow-Committee-member and Catholic assisted dying opponent Mrs Inga Peulich asked about the same thing (with Mr Mulino present) — “1,000 of those who have been accidentally euthanased in the Netherlands” — I literally put the chart up on the projection screen and explained it in full to the Committee until they had no more questions. The “1000” figure is the approximate rate prior to the Dutch Euthanasia Act, while the rate has dropped significantly since.
The evidence is irrefutable: it’s not like Mr Mulino was merely blissfully unaware of the relevant data contradicting his NVE ‘slippery slope’ claim. His minority report expressly overlooks this robust evidence and instead refers inapproriately to selective and outdated data that seemed to, but didn’t, support his argument.
Five major offences in a single citation: surely Mr Mulino’s report — far from ‘academic and rigorous’ — sets a new record?
A common religious thread?
The NVE ‘slippery slope’ claim is also popular amongst and spread by the Catholic Archdioceses of Melbourne,13 Sydney14 and Brisbane,15 as well as by other Catholic anti-assisted dying lobbyists such as Alex Schadenberg,16 Paul Russell,17 and Professor of Ethics at the Catholic University of Notre Dame Australia, Margaret Somerville.18
Indeed, Mr Mulino’s minority report appears amongst 11 Catholic responses against assisted dying law reform published by the Catholic Archdiocese of Melbourne (Figure 10).
Figure 10: Daniel Mulino’s minority report appears amongst Catholic responses on the Catholic Archdiocese of Melbourne’s website19
Indeed, Mr Mulino’s linked document doesn’t seem to emanate from his parliamentary office or from wider parliamentary services: the PDF file's metadata reveals that it was authored, electronically at least, by “mmacdonald”.
Calls to both Mr Mulino's electorate office and to the Parliament of Victoria confirm there is no "M Macdonald" at either. I did, however, find online one Matthew Macdonald, researcher and Executive Officer of the Catholic Archdiocese of Melbourne’s (CAM) Office for Life, Marriage and Family — in other words, the same organisation that published the list in Figure 10 containing the link to Mr Mulino’s minority report.
Mr Macdonald is also listed as the CAM's official contact person in its submission (#705) opposing assisted dying to the Victorian Parliament's inquiry into end of life choices.20 Both the CAM and Mulino reports also refer to a journal paper by Catholic doctor José Pereira,21 and neither report mentions the subsequent evidential rebuttal outlining why Pereira's claims were merely "smoke and mirrors".22 Even more curiously, the Pereira paper is included in Mr Merlino's minority report bibliography, though his report doesn't actually cite it as the CAM submission does.
The CAM parliamentary submission was authorised and signed by Episcopal Vicars Anthony Ireland and Anthony Kerin, who also appeared as witnesses before the parliamentary Committee, during which they told, as I've explained, a whopping great falsehood about Oregon.23
Conclusion
Contrary to Paul Russell’s enthusiastic claim that Daniel Mulino’s minority report provides a ‘rigorous’ case against assisted dying law reform, the report merely serves as further evidence of how those implacably opposed to assisted dying can cherry-pick, misunderstand and rather desperately clutch their way through their ‘evidence.’
Mr Russell is not an academic expert and one can understand his limited capacity to judge whether work is ‘scholarly.’ However, Mr Mulino holds a PhD in economics from Yale,* so it’s quite astonishing that he published a ‘researched’ report containing multiple major flaws, including outdated and cherry-picked data contrary to more recent, direct and relevant evidence of which he was specifically aware, actively inquired into and had explained and cited to him in full.
These anomolies beg the question: did Matthew McDonald or someone else at the Catholic Archdiocese of Melbourne write Mr Mulino’s report for him? Mr Mulino needs to explain himself, since regardless of who authoried it, he signed it off in his own name and is therefore ultimately responsible for it.
Given the multiple fundamental errors, the honourable course for Mr Mulino to pursue is to withdraw his minority report.
The question is: will he rise to the occasion?
Addendum: A missed opportunity for primary research
Mr Mulino — as well as Mrs Peulich who also wrote a minority report against assisted dying — declined to join other members of the parliamentary Committee on an official overseas fact-finding tour to jurisdictions where assisted dying is lawful. This was a critical opportunity for Committee members to directly quiz proponents, opponents, researchers, regulators, legislators and others with direct experience. It would have given them invaluable opportunities to directly examine and test assumptions, hypotheses and performance. How curious then that these two non-participataing Committee members each furnished a minority report opposing the majority recommendation to legalise assisted dying in Victoria.
---------------
§ The HOPE website is an initiative of the Australian Family Association (AFA), a faith-based organisation founded by Australia’s most famous Catholic, B. A. Santamaria. Mr Russell is a former Vice President of the AFA, and a former Senior Officer for Family and Life at the Catholic Archdiocese of Adelaide.
* While Mr Mulino holds a PhD and would be entitled to be addressed as “Dr”, his Parliamentary title is “Mr”.
Ganzini, L, Nelson, HD, Schmidt, TA, Kraemer, DF, Delorit, MA & Lee, MA 2000, 'Physicians' experiences with the Oregon Death with Dignity Act', New England Journal of Medicine, 342(8), pp. 557-563.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, 362(9381), pp. 345-350.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, 380(9845), pp. 908-915.
Bilsen, J, Cohen, J, Chambaere, K, Pousset, G, Onwuteaka-Philipsen, BD, Mortier, F & Deliens, L 2009, 'Medical end-of-life practices under the euthanasia law in Belgium', New England Journal of Medicine, 361(11), pp. 1119-1121.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, 23(3), pp. 198-204.
Francis, N 2015, Submission to the Parliament of Victoria Standing Committee on Legal and Social Issues on the Inquiry into End of Life Choices, DyingForChoice.com, Melbourne, pp. 51.
Parliament of Victoria 2015, Standing Committee on Legal and Social Issues inquiry into end-of-life choices: Witness-Mr Neil Francis, DyingForChoice.com, Melbourne, pp. 10.
Schadenberg, A 2013, Exposing vulnerable people to euthanasia and assisted suicide, Ross Lattner, London ON.
Russell, P 2015, Submission 926: Submission to the Victorian Legal and Social Issues Committee inquiry into end of life choices, HOPE, Melbourne, pp. 56.
Catholic Archdiocese of Melbourne 2015, Submission to the Legal & Social Issues Committee: Inquiry into end of life choices, Submission 705, Melbourne, pp. 16.
Pereira, J 2011, 'Legalizing euthanasia or assisted suicide: the illusion of safeguards and controls', Current Oncology, vol. 18, no. 2, pp. e38-48.
Downie, J, Chambaere, K & Bernheim, JL 2012, 'Pereira's attack on legalizing euthanasia or assisted suicide: smoke and mirrors', Current Oncology, vol. 19, no. 3, Jun, pp. 133-8.
Blog by Neil FrancisPosted on Sunday 6th August 2017 at 2:31am
The terminally ill are not choosing between life and death, but between two ways of dying, according to their own beliefs and conscience. Photo: Andrew Drummond/AAP
In Monday’s Herald Sun, Victorian Archbishops Philip Freier and Denis Hart, and Bishops Ezekiel, Suriel, Lester Briebbenow, Bosco Puthur and Peter Stasiuk published a half-page advertisement admonishing the Victorian government for its initiative to legalise assisted dying for the terminally ill, an ad similar to the one published by religious figures in 2008.
I have no quarrel with individuals of faith regarding their own private beliefs. However, the bishops’ attempt at public “leadership” through the advertisement is deserving of redress for its multiple fallacies.
The ‘abandonment’ fallacy
The bishops claimed that assisted dying “represents the abandonment of those who are in greatest need of our care and support”. On the contrary: to ignore the deeply-held beliefs and rigorously-tested wishes of people at the end of life is to abandon their values and critical faculties in favour of the bishops’ own religious dogma.
The ‘competition’ fallacy
The bishops demand there should be more funding for healthcare rather than assisted dying, fallaciously pitting one option against the other. The Victorian government is indeed increasing funding for palliative care. It’s also aiming to provide lawful assisted dying for when even the best palliative care can’t help – which Palliative Care Australia has acknowledged – giving lie to the faux competition.
The evidential fallacy
Contrary to the bishops’ false presumption that legalised assisted dying will decrease trust in “the treatment and quality of care” from doctors, scientific studies into attitude change show that more people trust doctors when assisted dying is legal. Patients can then talk openly about options, even if they decide against assisted death. The bishops have abandoned facts in favour of religious assumptions.
The equivalence fallacy
The bishops refer to assisted dying as “government endorsed suicide”. They fallaciously equate a reasoned, tested and accompanied decision for a peaceful assisted death in the face of a terminal illness, with the impulsive, violent, isolated and regrettable suicide of individuals (many of whom have mental health and substance abuse issues) who are failing to cope with problems that can be addressed.
However, while the latter are choosing between life and death, the terminally ill are choosing not between life and death, but between two different ways of dying, according to their own beliefs and conscience. Rigorous 2016 research from Australian National University shows that the vast majority (79%) of Victorians support assisted dying choice for the terminally ill (with just 8% opposed), clearly distinguishing it from general suicide.
Shame on the bishops for disrespectfully equating the two.
The inconsistency fallacy
They also argue that assisted dying ought to remain prohibited because within healthcare, “mistakes happen and the vulnerable are exploited,” and “that in spite of our best efforts, our justice system could never guarantee” no one would die by mistake or false evidence. However, as I’ve pointed out before, an identical hypothetical problem exists under the refusal of life-saving medical treatment, a statutory right that Victorians have enjoyed for nearly 30 years. The statute has only three “safeguard” requirements, yet even those only apply if the refusal is formally documented, but not if it’s verbal.
Further, the United States Conference of Catholic Bishops directs that patients may refuse treatment if it imposes “excessive expense on the family or community,” yet makes no mention of the hypothetical “vulnerability” of the patient to be persuaded so, nor directs any requirements to assess the veracity of the refusal.
In stark contrast, the Victorian proposal for assisted dying legislation contains more than 60 safeguards and oversights.
The bishops are at risk of ridicule for such a gargantuan flip-flop: supporting the refusal of life-saving treatment with little or no oversight, while vocally opposing assisted dying legislation that mandates an armada of protections.
The not-so-hidden agenda
The bishops’ methods are rather unsubtle – hoping that these arguments, erroneous but carefully crafted to avoid any religious connotations, will be accepted as non-religious. Yet religion is writ large across their plea: as signatories to the letter they are all clerics employed directly and centrally in the promotion of their religions.
The authority fallacy
They might also rely on their religious status to convey gravity and authority to their pleas. Yet as people paid to do a job, like anyone else, their titles grant them no special privileges in lecturing Victorians about how they should die in the face of a terminal illness.
According to the 2016 census, just 23% of Victorians identified as Catholic, 9% as Anglican, 0.5% as Lutheran, and the other bishops’ signatory denominations so small as to not appear separately in the government’s statistics. Combined, the bishops’ faiths represent around 33% of the Victorian population, while 32% of Victorians identify with no faith at all. Surely the bishops are not arguing that they’re speaking for these other Victorians, too?
But the bishops don’t represent the views of their own flocks, either. According to the 2016 ANU study, 89% of non-religious Victorians support assisted dying law reform, as do 78% of Victorian Catholics and Anglicans. Indeed, opposition to assisted dying exists mostly among those who attend religious services once a week or more often – that is, those who are frequently exposed institutional religious messages of opposition – yet who comprise just 12% of Australians and 11% of Victorians.
Minding their own flocks
Australians are abandoning religion in droves. For example, when Freier ascended to the top job of Anglican Primate of Australia in 2006, some 19% of Australians identified as Anglican (2006 census). A decade later under his leadership, the 2016 census showed a drop of about a third to just 13%, and in Victoria, his home territory, to just 9%.
Hart’s Catholic church has experienced a drop in affiliation too, and it’s likely to continue and accelerate as Australians react with shock and disgust to the extent of child sexual abuse that the royal commission has exposed from under his organisation’s “pastoral umbrella”.
In conclusion, rather than bishops lecturing the government and Victorians with fallacious and faintly desperate arguments about the choices they shouldn’t have at the end of life, attending to their own flocks may be more useful Christian leadership.
May their God go with them in that endeavour.
This article was originally published in The Guardian.
To add insult to injury, it flip-flops on its stance.
Never mind that the argument is contradicted by evidence
The Church’s favourite argument — already contradicted by scholarly analysis that curiously seems to be of no interest to the Church — is this: if people are given the choice of assisted dying, they will feel compelled to choose it, coerced by doctors, greedy relatives or others; subtly or otherwise.
No matter that health care workers routinely report that relatives usually try and persuade their dying loved one to endure yet another invasive and burdensome treatment; not dissuade them from it.
The flip-flop
If the Catholic Church were indeed genuinely concerned about coercion of ‘the vulnerable,’ then it would equally oppose the right to refuse medical treatment, particularly if the treatment were life-prolonging. But it doesn’t.
If granny might die as a result of refusing a particular medical intervention, then a doctor might persuade her to refuse in order to conserve medical resources. Or greedy relatives might persuade her so that they are relieved of the burden and expense of looking after her and gain earlier access to her estate.
As eminent legal scholar Gerald Dworkin has argued,1 if there’s a theoretical ‘slippery slope’ for assisted dying, it’s the same for the refusal of life-preserving medical treatment.
To hold different positions under the same risks is to flip-flop. That’s especially so when there are numerous safeguards built into assisted dying statutes, but currently few or none for the right to refuse life-preserving medical treatment.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
Local experience confirms risk is theoretical
In my home state of Victoria, where the right to refuse any unwanted medical treatment has been enshrined in statute for nearly three decades (the Medical Treatment Act 1988), how many prosecutions have there been under the Act’s provisions against inappropriate persuasion?
Precisely none. Not a single case. So much for the theory.
It all serves to highlight that the Catholic Church’s only real argument is that it believes that it’s morally wrong to deliberately hasten death. However, it avoids this argument because as a religious tenet, it doesn’t appeal to the masses.
Catholic directives
The Church’s flip-flop about ‘the vulnerable’ is not a one-off accident. Take for example the ‘Ethical and Religious Directives for Catholic Health Care Services’ published by the United States Conference of Catholic Bishops.2
The Bishops ‘direct’ that there is no obligation on patients to use disproportionate means of preserving life. They state that disproportionate means are:
“…those that in the patient’s judgement do not offer a reasonable hope of benefit or entail an excessive burden, or impose excessive expense on the family or the community.”
The Bishops further ‘direct’ that:
“The free and informed judgment made by a competent adult patient concerning the use or withdrawal of life-sustaining procedures should always be respected and normally complied with, unless it is contrary to Catholic moral teaching.”
Setting aside the Church’s hubris of dishonouring the patient’s choice if the Church disagrees, it would be theoretically easy for someone to persuade the patient that hope was not reasonable, that the burden would be too great, or that the cost to the family or society would be too high.
Suffering for our God’s (your own) good
On the next page, the Bishops expressly ‘direct’ that:
“Patients experiencing suffering that cannot be alleviated should be helped to appreciate the Christian understanding of redemptive suffering.”
That’s unqualified. So, if you’re atheist, agnostic, Jewish, Hindu, Muslim or even a Christian who believes assisted dying can be appropriate, as a patient in their institutions you are to be persuaded that suffering against your beliefs and wishes is ‘redemptive’ in the eyes of the Vatican’s version of a God.
In Australia in 2009, for the Office for Family and Life in the Catholic archdiocese of Adelaide, Mr Paul Russell argued in News Weekly that “there is a point to suffering” because:
“It’s about the profound connection that each and every life has to the incarnate God … We know that the sufferings we endure well are joined in some mysterious way to the sufferings of Christ.”
Pity any poor soul who doesn’t share Mr Russell’s views. Curiously, there is no mention of this underpinning belief in his anti-assisted dying blog, “HOPE.”
Invalid argument in any case
The Church’s argument that ‘the vulnerable’ will be ‘at risk’ from assisted dying laws — for example in the Victorian Bishops’ recent pastoral letter to the Catholics of Victoria opposing the upcoming assisted dying parliamentary Bill — is itself fundamentally invalid.
That’s because, as I’ve previously explained, it’s a circular argument: a logical fallacy.
A circular argument: We must ban yellow socks on Wednesdays or the 'vulnerable' will be 'at risk'.‘The vulnerable,’ by definition are those ‘at risk,’ and will still be so if we wear yellow socks on Wednesdays. Therefore, we should ban such bright footwear midweek — and anything else we happen to oppose — on the same basis.
Might anyone suggest that “we should ban religion because the vulnerable will be at risk of succumbing to extreme religious views”?
Will the Church change its mind?
The Catholic Church does change its mind from time to time, though its reforms are glacially slow.
Take, for example, its theory of limbo, a place on the doorstep of hell where, the Church claimed, babies go if they die before they’re baptised: that they’d be prevented from entering heaven. It would be hard to imagine a crueller worry to put into the heads of uneducated new parents.
But in 2007, after centuries of confidently promoting the theory, the Catholic Church decided that it was wrong and buried it.
Will it change its mind on assisted dying? Maybe, but don’t hold your breath.
Conclusion
The Catholic Church, reeling from its extensive failure to protect our most vulnerable — children — and notwithstanding some good individuals within, still presumes to morally lecture the rest of us with the logical fallacy of how ‘risky’ assisted dying legislation is supposed to be to ‘the vulnerable,’ while flip-flopping in support of refusing life-saving medical treatment under the same theoretical risk.
The Bishops’ rhetoric amply exposes their confected crisis against assisted dying as nothing but religious doctrine draped in faux secular garb… in reality a sheep in wolves’ clothing.
References
Dworkin, G, Frey, RG & Bok, S 1998, Euthanasia and physician-assisted suicide, Cambridge University Press, Cambridge, New York. pp.66ff
Blog by Neil FrancisPosted on Wednesday 21st June 2017 at 3:14am
More Dutch evidence contradicts Margaret Somerville's 'suicide contagion' theory
I’ve previously published an extensive analysis of how Professor Margaret Somerville, of the Catholic Notre Dame University of Australia, cherry-picked her way through select data that seemed to be (but wasn’t) consistent with her ‘contagion’ theory from assisted dying to the general suicide rate. I provided ample evidence from lawful jurisdictions that comprehensively contradicts her claim. I also published the summary in ABC Religion & Ethics.
Yet Somerville still says despite extensive real-world experience to the contrary, that “I believe that my [suicide contagion] statement will prove to be correct.”
She and her Catholic colleagues still hold onto several tenuous threads of information that might — just might — appear consistent with her theory, despite the truckloads of evidence to the contrary.
One of those tenuous threads is that the general suicide rate in the Netherlands has increased from 2008, around the same time that use of the Dutch euthanasia law also increased. (The general suicide rate previously fell as assisted dying rates increased.)
I reported official Dutch government statistics and expert financial reports to show that the unemployment rate explains most (80%) of the variation in the Dutch general suicide rate since 1960, and that the Netherlands was particularly hard-hit by the global financial crisis from 2008 — whereas neighbouring Belgium wasn’t and its suicide rate dropped as assisted dying numbers increased. Unemployment in hard times is a known significant risk factor for suicide.
Now, a detailed and peer-reviewed analysis of Dutch data recently published in the Netherlands Journal of Medicine throws more mud in the face of Somerville’s theory.1
The research looked at the Dutch assisted death and general suicide rates from 2002 through 2014, separately for each of the five Euthanasia Commission reporting regions.
Headline results of the averages for 2002–14 are shown in Figure 1.
Figure 1: The average assisted death rate (and suicide rate) as a percent of all deaths by region, 2002-14 Source: Koopman & Putter 2016
As you can see, Region 3, which includes Amsterdam, had by far the greatest assisted death rate (3.4%), compared with the other four regions (1.7% – 2.0%). Yet Region 3’s suicide rate at 1.2% was the same as Region 5 which had only half the assisted death rate of Region 3 (1.7% vs 3.4%). (The authors, unusually, expressed suicides as a percentage of all deaths rather than per 100k population.)
The results are the opposite of Somerville’s theory which says that Region 3’s general suicide rate should be much higher than (not the same as) Region 5’s.
Those figures are the average for 2002–14. It’s possible that the picture is a little different for the more recent years in which the assisted dying rate is higher.
To answer that question, I’ve retrieved official Dutch Government data and calculated the assisted dying rates and general suicide rates for 2014 alone, the most recent year for which all the data is available. I’ve also calculated the general suicide rate per 100,000 population, the more usual way of reporting and comparing suicide statistics. The results are shown in Figure 2.
Figure 2: The Dutch assisted death rate and general suicide rate by region for 2014 Sources: Euthanasia Commission annual reports, Dutch Government statistics
While region 1 (the far north) has the lowest assisted death rate (3.2% of all deaths), it has by far the highest general suicide rate (13.6 per 100k population).
The latest Dutch regional data shows the opposite of Margaret Somerville’s ‘suicide contagion’ theory, adding to the already extensive evidence against it.Conversely, region 3 (which includes Amsterdam) has by a very large factor the highest assisted dying rate (6.0% of all deaths), yet it has the second-lowest general suicide rate (10.3 per 100k population).
This latest empirical evidence is consistent with other extensive evidence I’ve published showing an inverse — or no — relationship between assisted dying rates and general suicide rates.
The question is whether Margaret Somerville and her Catholic friends will pay the slightest attention, or continue to rely on invalid, cherry-picked morsels of data that they think support their theory, but don’t.
References
Koopman, JJE & Putter, H 2016, 'Regional variation in the practice of euthanasia and physician-assisted suicide in the Netherlands', Netherlands Journal of Medicine, 74(9), pp. 387-394.
Blog by Neil FrancisPosted on Tuesday 13th June 2017 at 2:38am
The Age reports a 'gloves off' campaign of misinformation
Both the Herald Sun and The Age reported last week that religious anti-assisted dying crusaders are running a 'gloves off' campaign in Victoria.
Religious forces are gathering once again to attempt to thwart the views of the great majority of Victorians in favour of assisted dying law reform.
Matt Johnston in the Herald Sun quoted Paul Russell, a long-term figure in Catholic circles, and Greek Orthodox Bishop Ezekiel, in statements against assisted dying.
Farrah Thomazin in The Age quoted religious stalwarts Margaret Tighe of Right To Life, and the Australian Christian Lobby, in further statements against assisted dying.
The crux of the story is that 'pollsters' claim to have run a survey in Victoria. They refuse to be identified. They refuse to publish their methodology. And they refuse to publish all their results. Enough said.
They cherry-pick an item from their supposed poll to claim that 33% of Victorians who oppose assisted dying will change their vote against a supporting politician at the next election. They neglect to mention that only a tiny minority of Victorians actually oppose assisted dying. Their analysis is astonishingly superficial, even assuming they ran a proper, robust poll and didn't manufacture the numbers themselves.
They then use this tidbit of 'data' to put the fear of electoral defeat into politicians who will soon to face an assisted dying Bill in the Victorian Parliament.
What rubbish. Assisted dying (AD) opponents seem to be utterly shameless in misrepresenting and distorting cherry-picked data to push their religious agenda — which they pretend isn't religious.
The real situation in respect of AD is the exact opposite of their claims as I show in a proper, robust analysis of legitimate data, demonstrating that:
A massive 78.9% of Victorians support AD, with only a tiny 8.1% opposed. Strong supporters outnumber strong opponents by more than ten to one.
Significantly more supporters of AD believe that law reform is personally important, than opponents believe the status quo (no law) is personally important.
At a general election, far more Victorian voters will punish Members who oppose the AD Bill than will punish Members who support it (3.5 to 1 overall, 2.4 to 1 for the Liberal/National Coalition and 6.6 to 1 for Labor).
The co-sponsors of Victoria’s 2008 AD Bill were returned with greatly increased majorities (including relative to their party’s overall performance) despite campaigns against them by anti-AD crusaders.
So that Victorian politicians are not misled, I have forwarded my report to the Victorian Government's Cabinet and other selected members of Parliament.
The only way in which this campaign could be called 'gloves-off' is that opponents, lurking around with their shadowy misinformation, don't want to get bullshit on their mittens. Hands seem to be much easier to wash. And hide.
Fact file by Neil FrancisPosted on Thursday 25th May 2017 at 12:00am
Those actively opposing assisted dying laws are Australia's most religious. Photo: Donaldytong
A claim was recently made on ABC’s QandA that at least 70% of Catholics and Anglicans support assisted dying. The claim was challenged and a FactCheck prepared and vetted by scholars. They concluded that some but not all polls supported the statement. I show unambiguously that relevant polls do. I show further, as I have in the past, that opposition is largely associated with Australia's most religious.
In 2007, a Newspoll survey found that 74% of Catholics and 81% of Anglicans support assisted dying. The 2016 Australian Election Study (AES), run by scholars at Australian National University, found almost identical rates: 74% of Catholics and 79% of Anglicans. Although a majority of all religious denomination groups support assisted dying, opposition is highest among minor Christian denominations (Figure 1).
Figure 1: Attitudes toward assisted dying by major religious denominations Source: AES 2016. Note: Chr. = Christian
A significant majority of support for assisted dying was also found across all age groups, education levels, income levels, states, and major political party affiliations and religious denominations, with support amongst Australians overall at 77%.
Casting doubt
However, another poll cited in the FactCheck found far less support: the 2011 National Church Life Survey (NCLS). It found just 28% of Catholics and 25% of Anglicans supported assisted dying.
The problem with the NCLS poll is that it didn’t take a valid sample of Australian Catholics and Anglicans. It sampled mostly or only those who frequently attend religious services.
Views vary widely by attendance frequency
Figure 2 shows the level of support amongst the Australian public, by frequency of attending religious services. While just 2.4% of those who never attend religious services oppose assisted dying, 46.1% of those attending at least once a week oppose it.
Figure 2: Attitudes toward assisted dying by frequency of attending religious services Source: AES 2016
NCLS poll cannot answer the question
The NCLS results were even more negative than the AES ‘at least once a week’ results. That’s explained by the NCLS methodology. Firstly, occasional attenders were underrepresented, and non-attenders were excluded altogether. Secondly, more church employees (the most deeply committed and aligned with church policies) than others would have participated. Thirdly, responders may have felt pressured to toe the church line because the survey forms were collected by the churches themselves. And fourthly, those who disagreed with the church line would be less likely to participate.
ABC QandA question answered
So we can discount the NCLS poll because it was not suited to answer the question about all Australian Catholics and Anglicans.
On that basis, it is not only reasonable to say that “up to 70% of Catholics and Anglicans support assisted dying,” but to say that “at least 70% of Catholics and Anglicans support assisted dying.”
Religious connections of opposers
But, back to the opposition of assisted dying. AES data shows that 92% of those opposing and 94% of those strongly opposing assisted dying have a religious affiliation (self-identify with a religious denomination) or attend religious services. So, while a tiny minority of opposers had no religious affiliation nor attended religious services, almost all those opposing have a religious connection.
Frequent service attendance entrenches opposition
If we focus in on those who identify with a religious denomination and who disagree with assisted dying, we find that there’s a massive difference in opposition to assisted dying between the ‘at least once a week’ attenders and everyone else (Figure 3).
Figure 3: Frequency of attending religious services amongst those with a religious affiliation and who disagree with assisted dying Source: AES 2016
Not only are the majority of opposers weekly religious service attenders, but weekly attenders are more likely to be strongly opposed. This highlights the strong alignment with and commitment to religious teachings, which (with rare exceptions) oppose assisted dying.
If we define the most religious Australians as those who attend religious services monthly or more often and who self-identify with a religious denomination (“Regulars” in Figure 4), and who make up just 15.7% of the population, their attitudes are remarkably more opposed to assisted dying than all other Australians — by a factor of more than eleven to one.
Figure 4: Attitudes by religious service attendance plus denomination affiliation (“Regulars”) Source: AES 2016
Amongst the 84.3% of Australians who are not “Regulars”, almost all of them (85.7%) agree with assisted dying, and almost none of them (3.6%) disagree.
Demographic differences explained by religiosity
The variation in attitudes toward assisted dying by general demographics is largely explained by religiosity — defined here as ‘the frequency of attending religious services’.
For example, the increased opposition amongst older Australians is explained by their increased religiosity. The same applies to religious denomination affiliation (e.g. Catholics attend services more often than Anglicans), education, urban versus rural residence, and political party first preference.
Religiosity was the only variable that independently explained variations in opposition to assisted dying.
The double whammy — affiliation and attendance
Also informative is the comparison of those with or without a religious affiliation versus those who do and don’t attend religious services. (Australians fall into all four categories.)
Amongst those with no religious affiliation, people who do attend religious services are only slightly less likely (than those who don’t attend) to support assisted dying (-7%), and their difference in attitude is mostly to neutrality.
However, of those with a religious affiliation, people who do attend religious services are significantly less likely to support assisted dying (-27%), and the majority of their difference in attitude is opposition rather than neutrality.
Thus, those more deeply aligned with their religious denomination through service attendance are significantly more likely to oppose assisted dying.
Moderated by personal experience
The 2007 Newspoll study asked respondents if they had personal experience of someone close who was hopelessly ill and had wanted voluntary euthanasia.
Amongst those with no religious affiliation, this personal experience increased support for assisted dying by just 3.7%, because support was already very high: from 90.9% to 94.6%.
However, amongst those with a religious affiliation, personal experience increased support for assisted dying markedly by 15.2%: from 72.4% to 87.6%.
Thus, those attending religious services, yet with close, personal experience of hopeless illness with a desire for assisted dying, were significantly less likely to align with opposed religious doctrine.
The most religious are a small minority
With so much opposition amongst Australia’s most religious, why is overall support for assisted dying so high? It’s because Australia’s most religious are a small minority of the population.
Nearly half (48%) of Australians never attend religious services, two thirds (65%) attend less than once a year or never, and three quarters (75%) attend once a year or less, including never.
Those who attend religious services frequently (weekly or more often) comprise just 12% of the population, while those who attend regularly (monthly or more often which includes the weeklies) comprise 16%.
Religion in Australia has been declining for decades, and the fall is likely to continue (see Appendix A of the full report, here), meaning that support for assisted dying is likely to increase in the future.
Conclusions
I’ve previously demonstrated how all the signatories to a major anti-assisted dying advertisement were deeply connected with religion. The AES and other studies further our understanding of wider public attitudes toward assisted dying in Australia. They show that while a substantial majority of Australians support assisted dying, almost all the opposition to it is connected with religion, particularly amongst the most religious who are a small minority of the population.
Despite the religious connection of those opposed, there is ample, robust evidence that a great majority of Catholic and Anglican Australians support assisted dying, backing the claim made on national television.
Clergy opposing assisted dying are not representing the broader views of their flocks. Perhaps they may not see that as their role, and perhaps this misalignment of attitudes and beliefs is an example of why religion in Australia is declining.
However, reflecting the views of the great majority of the constituency is the role of politicians, who would do well to take note of this robust evidence of a significant majority of support for assisted dying.
“#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
Her just-published IAHPC ‘Concept Note’ railing against assisted dying,1 and summarised on the European Association of Palliative Care’s (EAPC) website,2confirms and amplifies precisely the point I made.
Now you’d think that an organisation with a name like ‘International Association for Hospice and Palliative Care’ would be a neutral organisation representing the world profession irrespective of the faith or personal spiritual beliefs of its members.
But you’d be quite wrong.
Nothing but Catholic doctrine
The IAHPC's musings extensively cite several Popes as the authorities on the subject of — and exclusively against — assisted dying. They expressly use the term "Table of authorities," which includes Popes. And who else?
Precisely nobody: no other faith, and no impartial scientific research, is cited. Just Popes.
She also writes:
“IAHPC wishes to encourage our partners to express clear support for faith based teachings on palliative care.”
“It is important to clarify this misinformation [about ‘stealth euthanasia’] with the authoritative teachings of the Church.”
“Hospice has always been faith based.” [As if ‘the way it’s always been’ is a sound argument for ‘the way it always should be.’ Perhaps we shouldn’t have moved from serfdom to democracy?]
“The Catholic Church began the medieval hospice movement, and can lead the modern palliative care movement.” [They curiously neglect to mention that the palliative care (not hospice) movement rose from Anglican roots in the UK, helpfully confirming that this broadcast is primarily about promoting Catholic religion, not palliative care.]
Shameless self-promotion
But Dr Pettus and the IAHPC’s Concept Note don’t stop there.
“The Word [sic] Day of the Sick (WDS) is a good opportunity to support faith based healthcare organizations.”
“Contact your parish to see if you can hold a small event…”
“Contact your local Catholic health care provider director to find out about…”
“Make an announcement at your local church…”
Gosh, I must have been mistaken. I thought World Day of the Sick was about… the sick!?
But Dr Pettus and the IAHPC commandeer it to shamelessly further the Catholic religious agenda amongst palliative care service providers.
An unexamined conflict of interest
It's deeply disturbing that someone holding the position of “Advocacy and Human Rights Officer” considers the beliefs and values only of the service provider (who she represents) in promoting the world day about sick people (who her organisation serves).
Palliative care organisations repeatedly state that they aim to deliver patient-centred care. But the world palliative care peak body's self-adoration exposes the worst of them: taking the opportunity of a day supposedly for the values and needs of sick patients, and using it to glorify their own particular (Catholic) religious tenets which are to be lauded over those of the patients they serve.
Most of the world is not Catholic, and in Australia at least, most Catholics disagree with Vatican doctrine on assisted dying.
How astonishing then to dictate that Catholic doctrine must prevail over everyone, including Protestants, Hindus, Buddhists, Jews, Muslims, agnostics, atheists and others. Dr Pettus and the IAHPC comprehensively fail to demonstrate any awareness or reflection of potential conflicts of interest in serving people of different faiths and beliefs.
Incomprehensible arrogance
There is little issue with the Catholic Church directing its own willing adherents as to how they might end their days.
But for one religious institution to seek to impose its views on everyone worldwide is incomprehensibly arrogant. I guess it's no surprise then that a Catholic Bishop recently admitted — at a Royal Commission inquiry into the extensive, ongoing and horrific abuse of children under the Church's pastoral care — that the Catholic Church is a "law unto itself".
It would be helpful if the Holy See reflected on the principle: is it legitimate for another faith to force its own views on the Vatican or on Catholic patients?
It would also be helpful if the International Association of Hopsice and Palliative Care reflected on respecting and serving the wider community rather than behaving like a subsidiary of the Holy See.
Conclusion
The IAHPC has provided its own unequivocal proof that it is religious conservatism behind organised opposition to assisted dying, with the Catholic Church at the front of the pack.
You’ll understand why I tweeted in response to Dr Pettus:
“.@kpettus @EAPCOnlus Thanks for confirming @Pontifex arrogance. Not once did you mention PATIENT’S PoV. All about YOU.” — Neil Francis
- - -
And furthermore
Parading ignorance
The IAHPC refers repeatedly to the treatment of ‘pain’ in its stand against assisted dying law reform. But pain is not amongst the leading reasons for assisted dying (it is a much less common reason). Key reasons are the inability to participate in any of life’s enjoyable activities, loss of independence and loss of dignity.
I guess the curious focus on ‘pain’ is understandable though, because the Vatican is very fond of the doctrine of double effect (DDE) — which the IAHPC specifically notes in Catholic Catechism 2279 although not by its DDE name, but rather bizarrely as “a special form of disinterested charity.”
The DDE posits that it’s OK for a doctor to administer high doses of analgesics to treat pain, even if an unintended consequence is to hasten the patient’s death. The Catholic Church treats this doctrine as uncontroversial, even though it remains controversial amongst other ethicists and philosophers: the principle says “it’s quite OK for a doctor to kill her patient, as long as she doesn’t really mean to.”
I would commend Dr Pettus and the IAHPC to do some proper research and understand the subject area more competently before pontificating (yes, intended meaning) further.
The smokescreen argument
The IAHPC also states that:
“No country or state should consider the legalization of euthanasia or PAS until it ensures universal access to palliative care services.”
That’s purely a smokescreen argument for two reasons. Firstly, the Concept Note also argues that assisted dying:
“both violate[s] the bond of trust within the profession of medicine, and undermine[s] the integrity of the profession and the dedication to safeguard human life.”
Setting aside the empirical falsehood of the statement, it furnishes the IAHPC a 'get-out-of-jail-free' card if and when palliative care becomes ‘universally’ available: it’s utterly irrelevant if that goal is reached because there’s a more fundamental objection behind it.
Secondly, it's an established fact that palliative care can’t always help, even when the best services are available. ‘Universal’ access won’t fix all the problems.
All these faux arguments are typical and common from religious opponents of assisted dying.
Blog by Neil FrancisPosted on Thursday 9th February 2017 at 9:53pm
You only have to look to understand who is campaigning against your right to choose an assisted death in the face of intolerable and unrelievable suffering.
A case in point is a massive advertisement published in both of Melbourne’s daily newspapers: News Corp’s The Herald Sun (right-wing) and Fairfax Media’s The Age (left-wing). The ad was published in 2008 when Victorian MLC Colleen Hartland introduced the Medical Treatment (Physician Assisted Dying) Bill into the State legislature.
The Catholic Archbishop of Melbourne, Denis Hart, also sent the advertisement as a letter to all members of the Victorian Parliament.1
So, who are the advertisement’s signatories? I’ve listed them all in Table 1.
Table 1: Signatories to the 2008 Victorian anti-assisted-dying advertisement
Rt Rev. Graham Bradbeer
Moderator, Presbyterian Church of Victoria
The Rev. Fr Graeme A. Michell, FSSM
Parish Priest, Anglican Catholic Parish of St Mary the Virgin, Melbourne
Rev. Ross Carter
Uniting Church in Australia
Pastor Graham Nelson
Senior Pastor, Life Ministry Centre
Rev. Dr Max Champion
National Chair of the Assembly of Confessing Congregations within the Uniting Church in Australia
Rev. David Palmer
Convenor Church and Nation Committee, Presbyterian Church of Victoria
Pastor Mark Conner
Senior Minister of CityLife Church
Rev. Greg Pietsch
President, Victorian District, Lutheran Church of Australia
Dr Denise Cooper-Clarke
Adjunct Lecturer, Ridley Melbourne Mission and Ministry College
Rabbi Dr Shimon Cowen
Director Institute for Judaism and Civilization
Very Rev. Dr Michael Protopopov
Dean - Russian Orthodox Church in Australia
Rev. Megan Curlis-Gibson
St Hilary’s Anglican Church, Kew
Marcia Riordan
Respect Life Office, Catholic Archdiocese of Melbourne
Archbishop Dr Philip Freier
Anglican Church of Melbourne
Metropolitan Archbishop Paul Saliba
Primate of Antiochian Orthodox Archdiocese of Australia, New Zealand & the Philippines
Imam Riad Galil
West Heidelburg Mosque
Member of the Victorian Board of Imams
Bishop Peter Stasiuk CSSR DD
Eparchy of Saints Peter and Paul of Melbourne, for Ukrainian Catholics in Australia and New Zealand
Rev. Father James Grant SSC
Chaplains Without Borders,
Melbourne Anglican Diocese
Dale Stephenson
Senior Pastor Crossway Baptist Church
Assoc. Professor Afif Hadj MB BS (Melb) FRACS
Director of Surgery, Director of Medical Training, Maroondah Hospital (A Monash University Teaching Hospital)
Pastor Peter Stevens
Victorian State Officer
Festival of Light Australia
Archbishop Denis Hart
Catholic Archdiocese of Melbourne
Dr Nicholas Tonti-Filippini
Associate Dean, JPII Institute for Marriage and Family Melbourne
Rev. Fr Geoff Harvey
Priest of the Good Shepherd Antiochian Orthodox Mission Parish, based at Monash University
Rob Ward
Victorian State Director Australian Christian Lobby
Assoc. Professor Rosalie Hudson
Aged Care & Palliative Care consultant/educator
Jim Zubic
President of Orthodox Chaplaincy Association
Peter McHugh
Senior Pastor Christian City Church, Whitehorse
Persons in blue: Career is religion
Almost all of them are religious by career
To save you a lot of time assessing who these people are, I’ve coloured in blue all the folks whose job it is to espouse religion — at least, their own hierarchy’s view of it.
That’s 27 of the 29 signatories who by career are intensely immersed in their own religious perspective of the world; established and promoted through institutional doctrine.
But what about the other two?
What about the other two signatories, Assoc. Prof. Afif Hadi and Assoc. Prof. Rosalie Hudson (in yellow)?
Notice that Prof. Afif Hadi’s entry lists only his surgery profession. Highly relevant, but not mentioned, is that he was President (previously Vice Chairman) of the Australian and New Zealand Board of Trustees, Antiochian Orthodox Archdiocese of Australia and New Zealand. As head of the Board of the Archdiocese, his religious signature is intimately entwined with another: Metropolitan Archbishop Paul Saliba, the Primate of the Antiochian Orthodox Archdiocese.
Assoc. Prof. Rosalie Hudson’s listing too, mentions only seemingly secular links. What is omitted is that she is or was Chair of the University of Divinity (a multi-faith religious institution) Human Research Ethics Committee, Secretary of the Uniting Church’s committee on bioethics, a member of the Interfaith Committee, and an Academic Associate at Charles Sturt University’s School of Theology.
Thus, both Prof. Hadi and Assoc. Prof. Hudson are also deeply rooted in religious faith. The point is not to make any criticism of their faith or practice, but merely to observe the deeply religious connections to opposing assisted dying law reform. It’s worth mentioning that both Hadi and Hudson do valuable charity work.
So, all of them are deeply religious
A pertinent question to ask is: ‘What proportion of the signatories are neutral, scholarly researchers who have studied the empirical evidence from jurisdictions where assisted dying is already lawful?’ Answer: None of them. Enough said.
And what proportion of the signatories to this anti-assisted dying advertisement are very deeply invested in organised religion? The simple answer is as usual: 100%,all of them.
Disconnected from their flocks
Critically, these career-religious fail to reflect the views of their own flocks. We know from repeated polls, for example, that three out of four Australian Catholics, more than three out of four Uniting Church members, and four out of five Anglicans (Church of England) support assisted dying law reform.
This kind of clerical disconnect from the contemporary will of the people is one of the key reasons Australians are deserting religion in droves, as successive censuses show.
Conclusion
The evidence is irrefutable. Those who are actively organised to oppose your right to choose an assisted death are deeply religious, even when they use seemingly secular arguments (more on those later).
They are entitled to their opinions for themselves. But what right do they have to deny the vast majority of Australians, who do not agree with their views, the right to choose?
To phrase it in the personal, why does the Catholic Archbishop of Melbourrne, Denis Hart, think it appropriate to demand that Mr Geoff Drummond, a Buddhist, should have suffered against his will at the end of life for the Archbishop's version of faith, rather than Mr Drummond's own spiritual beliefs? Why does Rabbi Shimon Cowen think it appropriate to demand that Mr Alan Rosendorff, a fellow Jew, should have suffered against his will at the end of life for the Rabbi's version of faith, rather than Mr Rosendorff's own carefully-considered and deeply-held views? And why does Imam Riad Galil think it appropriate to demand that Mr Peter Short, not a Muslim, should have suffered against his will at the end of life for the Imam's beliefs, rather than his own?
Perhaps hubris remains alive and well amongst religious conservatives?
-----
Declaration: In fairness to those mentioned in this article, I openly declare that I am agnostic.
References
Bradbeer, G, Rt Rev., Carter, R, Rev., Champion, M, Rev. Dr, Conner, M, Pastor, Cooper-Clarke, D, Dr, Cowen, S, Rabbi Dr, Curlis-Gibson, M, Rev., Freier, P, Archbishop Dr, Galil, R, Imam, Grant SSC, J, Rev. Fr, Hadj, A, Assoc. Prof., Hart, D, Archbishop, Harvey, G, Rev. Fr, Hudson, R, Assoc. Prof., McHugh, P, Michell, GA, Rev. Fr, Nelson, G, Pastor, Palmer, D, Rev., Pietsch, G, Rev., Pietsch, M, Protopopov, M, Very Rev. Dr, Riordan, M, Saliba, P, Metropolitan Archbishop, Stasiuk, P, Bishop, Stephenson, D, Stevens, P, Pastor, Tonti-Filippini, N, Dr, Ward, R & Zubic, J 2008, Reject physician assisted dying - An open letter to Victorian MPs, Catholic Archdiocese of Melbourne, viewed 13 Jun 2008, http://www.cam.org.au/Euthanasia.aspx.
Blog by Neil FrancisPosted on Thursday 3rd November 2016 at 10:05pm
Notre Dame University welcomes Professor Margaret Somerville via its website.
In two opinion pieces recently published in the ABC’s conservative Religion & Ethics blog,1,2 Margaret Somerville, Professor of Bioethics at Notre Dame University, railed against marriage equality law reform using reasoning that I contend fails not only appropriate standards of ethics argument but indeed her own stated standards. Here’s why.
Railing against careful and reasoned language
In two ABC opinion pieces, Margo (as she refers to herself) railed extensively against the term ‘marriage equality,’ arguing that it ought to be referred to instead as ‘same-sex marriage.’ She volunteers that the real motive for her preferred term is that in her opinion fewer people will support ‘same-sex’ marriage than will support ‘equality’ of marriage.
Margo quite overlooks the fact that some folks deliberatively eschew gender identity or are asexual, yet may wish to honour a loving, life-long relationship through marriage. There’s also the issue of a change of gender identity within marriage, not just when entering into marriage.
The goal of Australian marriage law reform is a single, revised Act which articulates a uniform, equal set of provisions for marriage regardless of sexual orientation or gender identity: not a separate Act which permits a different version of marriage only for same-sex-attracted people.
Therefore, ‘marriage equality’ is indeed an appropriate expression for revised legislation while ‘same-sex marriage’ is less so.
“But what about the children!?”
Margo also railed extensively against marriage equality because, she claims, marriage is primarily about the rights of children, not the married couple.
However, the Marriage Act3 makes no assumptions about the marriage being for the purpose of producing children. Indeed, this would be foolish as it would preclude infertile couples from marrying. Here’s the entire definition of marriage under the Act:
“Marriage means the union of a man and a woman to the exclusion of all others, voluntarily entered into for life.” — Marriage Act 1961 (as amended)
Sure, the Act does have a couple of things to say about children, but in relation to the status of a legally adopted child, and child ‘legitimacy’ (which confers rights to use the family name and inherit titles, for example).
While the Act provides largesse for religious marriage celebrants to include any wording they deem appropriate (and which might cover the subject of procreation) in a marriage service, the minimum required civil celebrant wording is:
“I call upon the persons here present to witness that I, (first and last name), take thee, (first and last name), to be my lawful wedded wife/husband.” — Marriage Act 1961, S45(2) [or words like it]
No mention of children there, either. Section 1A.3 of the Marriage Regulations4 requires a marriage celebrant (religious and civil alike) to recognise “the importance of strong and respectful family relationships.” Notice again the absence of the presumption of producing children.
No necessary connection between children and marriage
Separate State and Territory Acts provide for the recognition of de facto relationships, over which the Commonwealth has no special jurisdiction. While recognised by the state these relationships are legally distinct from marriage.
In terms of unions that Australians willingly establish, Australian Bureau of Statistics data shows that:5
Around three quarters of marriages are now conducted by a civil celebrant rather than a religious one; and
Around one third of all Australian births are now to non-married partners.
It’s obvious that many marriages are now non-religious, that they can be childless, and, conversely, that many children are born in the absence of marriage. There is no necessary relationship in either direction between marriage and children that underpins Margo’s contentions.
No necessary link to assisted reproduction, either
Margo then goes on to rail against assisted human reproduction (surrogacy, gamete donation and IVF), complaining that non-hetero married couples would have to ask for such help to produce children. But, like the child argument itself, this is not unique in any way to marriage. De facto couples and even single women can ask for reproductive assistance, as can infertile hetero couples within marriage. As with children, assisted reproduction and marriage are not uniquely entwined as Margo wrongly argues: they are separate in law and practice even if the link is critical to some couples.
Why the confected 'necessity'?
So why then, does Margo go to such lengths to instil ‘children’ as central to the purpose of marriage? A potential explanation is that her expressed views, while reflecting neither law nor practice, are consistent with her Catholic faith. Catholic tradition is very deeply steeped in the notion that marriage is primarily for the purpose of procreation.
In her 2015 Bird on an Ethics Wire book, Margo invokes the 'would-if-they-could' defence for opposite-sex couples who want to marry but are intfertile (while remaining mute about married couples who expressly don't want children). She fails to articulate any sound reason as to why this is a different 'would-if-they-could' argument from same-gendered or non-gendered partners, except to argue, offensively, that same-sex partners are socially infertile for “lack of an opposite-sex partner.” In her ABC opinion pieces she simply says the hetero version is “symbolic.” Curiously for an ethicist, she fails to reflect on who gets to decide which are valid symbols and whether any symbolism ought to be mandatory for everyone.
Margo asserts that marriage between opposite-sex partners is ‘traditional.’ I say, good on her for personally sticking to a tradition she thinks important: but ‘tradition’ is a poor foundation for continuing to impose historical views on Australians who are not Catholic nor any longer support those views… which is the great majority of us.
The bogeyman argument
Margo then makes vague claims that marriage equality ‘takes away children’s rights’ and causes ‘harms.’ The ‘harm’ she does articulate is the “right to know one’s biological parents.” She speaks of anonymous gamete donation, but fails to note that it occurs equally both inside and outside of — and therefore isn’t conditioned by nor conditions — marriage. Therefore, any “right to know one’s biological parents” is, like children themselves and assisted reproduction in general, entirely independent of the marital status of the parents and is of no special force or relevance in marriage equality debates.
The not-as-good-as-heteros argument
Margo then promotes the importance of the “complementarity in parenting between a mother and father,” with the innuendo that same-sex parents are at least a much lesser standard for raising children, if not unsuitable altogether. Let’s examine this hoary old chestnut, particularly in relation to ‘expert’ evidence Margo proffered in a USA Court case.
Court assessment of Margo’s ‘evidence’
Historically, Iowa’s statute §595.2 restricted marriage to between only a man and a woman. A series of Iowa Court cases overturned that limitation in 2006–9. Margo and two of her colleagues from McGill University’s School of Religious Studies were advanced to the court as ‘expert witnesses’ against the reform, in relation to the ‘perils’ of marriage equality including the ‘harms’ to children. Here’s what the Iowa District Court concluded:6
“Though they may have expertise in certain areas, such expertise is insufficient to qualify Ms Somerville [and her two colleagues from the School of Religious Studies] to answer the particular questions that they are asked. Though these experts desire to make statements regarding gender, results of same-sex marriage on children and the universal definition of marriage, they do not appear to possess expertise in relevant fields such as sociology, child development, psychology or psychiatry. Ms Somerville specifically eschews empirical research and methods of logical reasoning in favour of ‘moral intuition.’ She has no training in empirical research and admits having no knowledge of existing social science research relevant to this case. She concedes that her views do not reflect the mainstream views of other ethicists.”
and
“The views espoused by these individuals appear to be largely personal and not based on observation supported by scientific methodology or based on empirical research in any sense.”
and
“…the Court concludes that these individuals are not qualified to testify as experts regarding the issues in this matter.”
The Court then expressly identified substantive harms that accrue to non-heterosexual partners through denial of marriage.
The case then went to Iowa’s Supreme Court. In a unanimous decision, the Supreme Court upheld the District Court’s determination, noting that:7
“The research appears to strongly support the conclusion that same-sex couples foster the same wholesome environment as opposite-sex couples and suggests that the traditional notion that children need a mother and a father to be raised into healthy, well-adjusted adults is based more on stereotype than anything else.”
and
“Many leading organizations, including the American Academy of Pediatrics, the American Psychiatric Association, the American Psychological Association, the National Association of Social Workers, and the Child Welfare League of America, weighed the available research and supported the conclusion that gay and lesbian parents are as effective as heterosexual parents in raising children.”
and
“For example, the official policy of the American Psychological Association declares, ‘There is no scientific evidence that parenting effectiveness is related to parental sexual orientation: Lesbian and gay parents are as likely as heterosexual parents to provide supportive and healthy environments for children.’”
So much for Margo’s ‘authority’ on the subject of marriage equality.
Those interested in a thorough rebuttal of Margo’s arguments against marriage equality might be interested to read papers by Scoff F. Woodcock of the University of Victoria (BC), an Associate Professor specialising in normative and applied ethics,8 and Timothy F. Murphy of the University of Illinois, Professor of Philosophy in the Biomedical Sciences specialising in professional ethics, assisted reproductive technologies, medicine and sexuality.9 Both these Professors hold earned doctorates in philosophy; whereas Margo, according to her own biography, holds earned academic qualifications in pharmacy and law, but none in philosophy or ethics.
The importance of relevant and persuasive facts
In an important recognition, a highly-published ethicist once wrote that:
“We sometimes overlook the importance of having good facts in dealing with ethical issues. This is a serious mistake. Good facts (including, if necessary, research to establish them) are essential to good ethics, which, in turn, is essential to good law.” and “Good ethical and legal ‘facts’ start with primary sources that are up to date and accurate.” [Italics are original]
That ethicist was… Margo Somerville.10 My view is that Margo has failed to live up to her own standards by getting some fundamental facts expressly wrong and misrepresenting others with innuendo whilst failing to mention readily-available and widely-agreed facts that contradict her thesis.
Also surprising is that she continues to opine against marriage equality law reform in Australia using the same opinions that were publicly and expressly rejected by a USA court; the same opinions that have been insightfully dissembled and rebutted by appropriately-qualified academics via analyses published in professional peer-reviewed journals.
Conclusion
An Iowa Court has determined that Margo Somerville’s views on marriage equality are largely personal and eschew empirical research and methods of logical reasoning in favour of ‘moral intuition.’ (More on ‘moral intuition’ in another blog.) Further, they are at odds with readily available research evidence. Her opinions then are not founded on scholarly verification and fail to reflect the highest standards of thought and deduction.
I firmly believe that Margo is entitled to her opinions. However, it is my view that appeals for her marriage equality opinions to be acclaimed on the basis of the authority bias — as “Professor of Ethics at Notre Dame University” and “a preeminent public intellectual in Bioethics” — are unjustifiable.
And if the ABC chooses to publish any more of Margo’s nonsense about ‘the perils of marriage equality to children,’ I might just ask for a refund of my twelve cents a day.*
-----
Up next: Who is Margo Somerville? Up later: Why is she so comprehensively wrong on assisted dying law reform?
* The ABC (Australian Broadcasting Corporation) is the nation’s public broadcaster and advertises that it provides its services for a mere twelve cents a day from each of the country’ residents.
Footnote: yet another fundamental (and simple) fact wrong
You’d think that being an accomplished Commonwealth legal scholar that Margo would understand the fundamental structure of Commonwealth legislatures.
But in her ABC missives against marriage equality, she concluded by remarking that same-sex couples often lament the lack of marriage equality “…such as we saw in the anguish Senator Tim Wilson manifested in his maiden speech in the Senate.” Here’s a photo of Tim Wilson delivering that speech:
Tim Wilson delivers his maiden speech in Parliament. Video still: ABC News
In Commonwealth countries, the upper house (Australia, federal: Senate) is fitted out in red (the colour of royalty and cardinals), while the lower house (Australia, federal: House of Representatives) is green (the colour of ‘common’ fields).
Immediately evident from glancing at his maiden speech for a mere millisecond is that Mr Wilson is not a Senator: all the livery is green. He is MHR for the Victorian Division of Goldstein, not a Senator for the State of Victoria.
The Canadian federal Parliament’s green House of Commons and red Senate (Margo has recently returned to Australia from decades in Canada) Photo: Mightydrake
It’s bewildering then that when Margo saw Mr Wilson’s maiden speech she utterly failed to establish which house he was in, nor took the trouble to examine or test her assumptions before publishing her ‘expert’ opinion about it online.
Iowa District Court for Polk County 2007, Katherine Varnum et al. v. Timothy J. Brien, CV5965, pp. 63.
Supreme Court of Iowa 2009, Katherine Varnum et al. v. Timothy J. Brien (Polk County), SCC No. 07-1499, Des Moines, pp. 69.
Woodcock, S 2009, 'Five reasons why Margaret Somerville is wrong about same-sex marriage and the rights of children', Dialogue-Canadian Philosophical Review, 48(4), pp. 867-887.
Murphy, TF 2011, 'Same-sex marriage: Not a threat to marriage or children', Journal of Social Philosophy, 42(3), pp. 288-304.
Somerville, MA 2014, Death talk: The case against euthanasia and physician-assisted suicide (2nd Ed.), 2nd Ed. edn, McGill-Queen's University Press, Montreal.
The F filesPosted on Friday 14th October 2016 at 1:21am
BMA House in Tavistock Square, London, home to the British Medical Association since 1925.
The British Medical Association (BMA), in the latest incarnation of its policy on assisted dying (AD), insists that AD must not be legalised in the UK. I argue that its indefensible stance reveals ignorance, incoherence and hubris. It fails to respect the true range of views amongst UK doctors. I expose the comprehensive rot.
The BMA categorically states in its July 2016 policy update on assisted dying:
“The BMA policy … insists that voluntary euthanasia [and] physician-assisted suicide should not be made legal in the UK.” — British Medical Association1
BMA comprehensively out of touch
The BMA claims to represent UK doctors—though fewer than half are members. What is the empirical evidence for UK doctor attitudes toward assisted dying?
In a 2009 survey,2 35% said that AD should definitely or probably be legalised. The same study also found that 35% of UK doctors said AD should definitely not be lawful even in cases of terminal illness. That is, the stance of just 35% of UK doctors was identical to the BMA’s—insisting that it not be lawful, while an equal proportion thought AD could be legalised. “Greater religiosity” was the strongest correlative factor with opposition to lawful AD.
Indeed, numerous studies have found a substantial minority of UK doctors in favour of lawful AD, including results approaching equality with opponents.3 Even a survey commissioned by the UK Catholic Medical Association in 2003 found around 25% of UK doctors in favour of AD and who would practice it if legalised.4
UK doctor support for AD, then, is substantial and hardly restricted to a mere handful of fringe-dwelling medical crackpots.
Ignorant and disrespectful BMA stance
It is untenable that the BMA unilaterally ‘respects’ the views of 35% of UK doctors at the same time as expressly disrespecting the views of another significant cohort. Perhaps as in general politics, its power base is more heavily populated with religious souls: those who have a deeper interest in shaping what options others do and don’t have?
Appalling and trivialised ‘rationale’
Let’s take a look at the five moribund reasons the BMA offers in defense of its institutional opposition to AD and see how they use flapdoodle, fudge, fiction, fear-mongering, flip-flop and hubris to ‘advance’ their position.
“Current BMA policy firmly opposes assisted dying for the following [five] key reasons:”
1. Permitting assisted dying for some could put vulnerable people at risk of harm.
Flapdoodle. Firstly, as I have explained before, the “vulnerable at risk” argument is a rhetorical sham. People ‘at risk’ are by definition ‘vulnerable,’ and would still be so if we wore yellow socks on Wednesdays or outlawed pizza. It has nothing to do with AD being legalised or not.
Fudge. Secondly, the BMA ignores repeated reviews published in the professional literature indicating that supposed harms have not eventuated in jurisdictions with lawful assisted dying. Indeed, the quality of medical practice has improved.
Flip-flop. And thirdly, if ‘risk of harm’ was a sufficient condition to deny patients a particular option, we must equally ban the right to refuse life-saving medical treatment (no matter how unwanted or burdensome) because greedy relatives eyeing off the estate might convince the dying patient to refuse. It’s incoherent to oppose assisted dying, but to support refusal of treatment (as the BMA does), in the face of this identical possibility.
2. Such a change would be contrary to the ethics of clinical practice, as the principal purpose of medicine is to improve patients’ quality of life, not to foreshorten it.
Fudge. Medicine has a number of primary purposes. Relief of suffering is one.5 That may come into conflict with another purpose, “the avoidance of premature death and the pursuit of a peaceful death” (which itself has internal conflicts). A dying individual may herself believe that an AD would not be premature, and whose peaceful nature is vastly preferable to continued intolerable and unrelievable suffering.
3. Legalising assisted dying could weaken society's prohibition on killing and undermine the safeguards against non-voluntary euthanasia. Society could embark on a 'slippery slope' with undesirable consequences.
Fear-mongering. Non-voluntary euthanasia (NVE) is currently illegal. It remains illegal even when AD is legalised. The BMA therefore incoherently conjectures that NVE doesn’t occur while it’s illegal (before AD legalisation), but might occur while it is still illegal (after AD legalisation).
Fiction. There are no current ‘safeguards’ against NVE as the BMA statement implies. It is practiced in secret. There are no statutory requirements or reporting standards as there are for AD (where legal). Research clearly demonstrates that NVE occurs everywhere, including the UK. Further, the rate of NVE has significantly decreased in the Netherlands and Belgium since their AD statutes came into effect.
4. For most patients, effective and high quality palliative care can effectively alleviate distressing symptoms associated with the dying process and allay patients' fears.
Flapdoodle. The BMA says “effective … palliative care can effectively alleviate…”: another circular, self-‘proving’ argument.
Hubris. The BMA acknowledges here—as unarguably established in the professional literature—that palliative care can’t help everyone. And that’s precisely what assisted dying law reform is about: for people that palliative care can’t help. But the BMA brushes them under the carpet.
5. Only a minority of people want to end their lives. The rules for the majority should not be changed to accommodate a small group.
Flip-flop. In ‘reasons’ 1 and 3 above, the BMA speculates that too many people will die if AD is legalised. Here is it arguing that too few will. Which is it? Too many or too few? The argument also ignores the international evidence that dying individuals (and their loved ones) experience profound relief merely from knowing that AD is available, even if they don’t pursue it. That itself is good palliative care.
Hubris. And if “not changing the majority's rules to accommodate a small group” were a gold standard as the BMA argues, then there would be no leglisation to (a) ensure facilities access to people with a disability, (b) outlaw discrimination on the basis of race or religion, or (c) allow same-sex marriage: all enshrined in law in the UK.
Hubris argues for ignoring the BMA itself
If, as the BMA argues, we should override the wishes of a group on the basis of its small size, it’s pertinent to consider the size of the UK doctor population: around 0.4% of the total. By comparison, in jurisdictions where AD is legal, around 0.3% (Oregon) to 3.8% (Netherlands) ultimately choose an assisted death.
If we are to ignore 0.3%–3.8% of the population because it’s ‘too small,’ we must equally ignore 0.4% of it. This, by the BMA’s own argument, would be reason to force it to support AD because that’s what the majority (UK population) favour. After all, “the rules for the majority should not be changed to accommodate a small group [of doctors].”
Of course most of us recognise, unlike the BMA, that this is not a ‘popularity contest.’ A stance of neutrality would demonstrate respect for deeply-held views across the spectrum.
Conclusion
The British Medical Association demonstrates profound ignorance about the available evidence, and about UK doctor attitudes. It resorts to fear-mongering speculation, fudge, fiction, flapdoodle, flip-flop and hubris to maintain its indefensible opposition to assisted dying.
The BMA’s stance does a great disservice to the British people. It’s an embarrassment to professional doctors regardless of their stance on assisted dying. The policy deserves to be entirely scrapped, and one of neutrality adopted in its place.
Seale, C 2009, 'Legalisation of euthanasia or physician-assisted suicide: survey of doctors' attitudes', Palliative Medicine, 23(3), Apr, pp. 205-212.
McCormack, R, Clifford, M & Conroy, M 2011, 'Attitudes of UK doctors towards euthanasia and physician-assisted suicide: a systematic literature review', Palliative Medicine, 26(1), pp. 23-33.
Catholic Medical Quarterly 2003, 'Euthanasia and assisted suicide: Results of survey of doctors attitudes', Catholic Medical Quarterly, May, pp. 1-3.
Hastings Center Report 1996, 'The goals of medicine. Setting new priorities', The Hastings Center Report, 26(6), pp. S1-27.

 Figures 1 and 2 (of Mr Mulino’s minority report): Assisted deaths in Belgium and the Netherlands
Figures 1 and 2 (of Mr Mulino’s minority report): Assisted deaths in Belgium and the Netherlands Figure 3: The full Netherlands data
Figure 3: The full Netherlands data Figure 4: Rate of assisted dying as a percent off all deaths in the Netherlands and Belgium 2003–2015
Figure 4: Rate of assisted dying as a percent off all deaths in the Netherlands and Belgium 2003–2015 Figure 5: Rate of assisted dying in the three lawful Benelux countries
Figure 5: Rate of assisted dying in the three lawful Benelux countries Figure 6: Netherlands total and assisted deaths for different periods
Figure 6: Netherlands total and assisted deaths for different periods Figure 7: The paper Abstract articulates exactly the opposite of Mr Mulino’s claim
Figure 7: The paper Abstract articulates exactly the opposite of Mr Mulino’s claim Figure 8: Table 2 from the 2003 study Mr Mulino cites
Figure 8: Table 2 from the 2003 study Mr Mulino cites Figure 9: Longitudinal NVE rates in the Netherlands, Belgium and the UK
Figure 9: Longitudinal NVE rates in the Netherlands, Belgium and the UK Figure 10: Daniel Mulino’s minority report appears amongst Catholic responses on the Catholic Archdiocese of Melbourne’s website19
Figure 10: Daniel Mulino’s minority report appears amongst Catholic responses on the Catholic Archdiocese of Melbourne’s website19

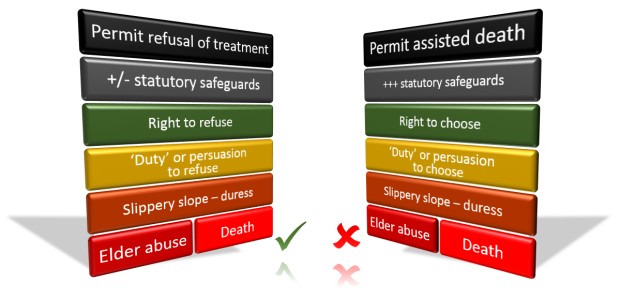 The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
 Figure 1: The average assisted death rate (and suicide rate) as a percent of all deaths by region, 2002-14
Figure 1: The average assisted death rate (and suicide rate) as a percent of all deaths by region, 2002-14 Figure 2: The Dutch assisted death rate and general suicide rate by region for 2014
Figure 2: The Dutch assisted death rate and general suicide rate by region for 2014

 Figure 1: Attitudes toward assisted dying by major religious denominations
Figure 1: Attitudes toward assisted dying by major religious denominations Figure 2: Attitudes toward assisted dying by frequency of attending religious services
Figure 2: Attitudes toward assisted dying by frequency of attending religious services Figure 3: Frequency of attending religious services amongst those with a religious affiliation and who disagree with assisted dying
Figure 3: Frequency of attending religious services amongst those with a religious affiliation and who disagree with assisted dying Figure 4: Attitudes by religious service attendance plus denomination affiliation (“Regulars”)
Figure 4: Attitudes by religious service attendance plus denomination affiliation (“Regulars”)
 “#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
“#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
 Tim Wilson delivers his maiden speech in Parliament. Video still: ABC News
Tim Wilson delivers his maiden speech in Parliament. Video still: ABC News The Canadian federal Parliament’s green House of Commons and red Senate (Margo has recently returned to Australia from decades in Canada) Photo: Mightydrake
The Canadian federal Parliament’s green House of Commons and red Senate (Margo has recently returned to Australia from decades in Canada) Photo: Mightydrake