To represent a thing or situation as considerably more sinister or dangerous than it is when assessed objectively using evidence and balanced evaluation.
Blog by Neil FrancisPosted on Monday 13th November 2017 at 6:28pm
The deeply-flawed Jones & Paton, and Kheriaty articles purporting to show suicide contagion.
In the ongoing political campaign against assisted dying law reform, opponents have spread one piece of egregious misinformation after another. One of the most common is supposed “suicide contagion” from assisted dying laws to general suicide, a theory popularised by Catholic Prof. Margaret Somerville. Despite the nonsense of her claim being comprehensively exposed, she still believes that her opinion “will prove to be correct.” Two journal papers published in 2015 purported to, but didn't, establish suicide contagion in Oregon and Washington states.
Assisted dying law reform opponents are still relying on a 2015 paper by Catholics David Jones and David Paton, bolstered by a glowing editorial of it written by Catholic psychiatrist Aaron Kheriaty, published in the Southern Medical Journal, as continued ‘proof’ of suicide contagion theory, at least in respect of USA states Oregon and Washington (since data from other lawful jurisdictions contradicts the theory).
Jones & Paton’s article reported the use of econometric modelling to test for ‘suicide contagion’ from Oregon and Washington’s Death With Dignity Act (DWDA) laws. But, in an exposé to be published this week, no fewer than ten ‘deadly sins’ of the study are peeled back to reveal the rot within.
The very deep flaws and biases of the original articles include:
Cherry-picking information from cited sources to argue their case, while omitting information from the same sources that contradicted their case;
Including test and control subjects whose consequence was likely to maximise the likelihood of finding a positive association;
Demonstrating a poor understanding of suicide and its risk and protective factors and failing to control for most confounding effects in their econometric model ‘pudding’;
Overegging the “causative suicide contagion” interpretation when no correlation between assisted dying and general suicide rates was found; and
Failing to use direct, robust and readily-available evidence that showed their study couldn’t possibly have hoped to return scientifically valid “contagion” proof.
The USA’s National Violent Death Reporting System (NVDRS), of which Oregon is a founding member, shows that even if “assisted dying suicide contagion theory” were true, fewer than 2 of 855 Oregon “total suicides” in 2014 could have been attributed to “contagion” from DWDAs.
Further, both Oregon and Washington state rankings for suicide rates have improved, not deteriorated, since their DWDAs came into effect, while the suicide ranking for a relevant control state — Oklahoma — has deteriorated substantially over the same time.
Ultimately, through numerous and deep methodological flaws, the Jones, Paton and Kheriaty articles reveal a bias to promote “assisted dying suicide contagion theory” while ignoring the robust evidence from multiple lawful jurisdictions, including in their own ‘study,’ that contradict it.
The exposé, titled “The ten deadly sins of Jones, Paton and Kheriaty on ‘suicide contagion’,” will be published by DyingForChoice.com later in the week.
Blog by Neil FrancisPosted on Friday 13th October 2017 at 10:11am
The Guardian reports a fracas within the Anglican church over a $1m political expenditure.
Anglican and Catholic bishops seem to be going out of their way to alienate their constituencies, including in respect of voluntary assisted dying and marriage equality law reform. As a result, the writing on the wall is writ large for the continued decline of religion in Australia.
Many Australian clerics are trying their hardest to foil Parliamentary attempts to drag Australia into the 21st century on social policy. They seem to care little for the ongoing demise of their own constituencies.
Religion declining since the 1960s
Religious affiliation in Australia has been declining consistently since the 1960s, consecutive Australian Bureau of Statistics (ABS) census figures show (Figure 1). At the 2016 census, somewhat more than half (60%) of all Australians claimed a religion. More Australians than ever before identified as ‘no religion’ — for the first time ever a larger group than any single religious denomination.
Figure 1: Australian religious affiliation by census year Source: ABS
Weak religious commitment
Not only has religious affiliation been dropping, but the nature of the affiliation is weak (Figure 2). Amongst the two largest religious denominations, a quarter of Catholics (26%) and nearly half of Anglicans (47%) are Notionals: that is, they identify with the denomination but never attend religious services. More than half of Catholics (52%), and four in ten Anglicans (41%), attend religious services only occasionally (Occasionals: several times a year or less often).
Figure 2: Australian denominations and Australian religious identity (ARI-6) Source: Australian Election Study (AES) 2016
Just 22% of Catholics and a mere 12% of Anglicans demonstrate commitment to their denomination through dedicated service attendance (Regular = monthly or more often, and Devout = weekly or more often).
The picture is particularly grim for the Anglican church, dominant in Australia from Federation until the 1960s. With both a deeply impoverished affiliation rate in 2016 (13.3%), and just 12% of the flock dedicated to service attendance, a miniscule 1.6% of Australians are committed Anglicans.
The picture is only slightly better for the Catholic church. With 22.6% affiliation in 2016, and 22% of those committed to service attendance, it's a slightly larger but still damningly small 5.0% of Australians who are committed Catholics. Further, the Catholic church’s affiliation may be significantly lower at the next (2021) census, as Australians vent their dismay and disgust at how badly it’s handled the scourge of child sexual abuse that’s occurred under its ‘pastoral umbrella.’
Hollow ‘leadership’
Across all religious denominations, just 16% of Australians are committed to their denomination — Regular or Devout religious service attenders — while 30.1% Reject religion altogether.
And yet those at the head of their ships of faith still demand that we listen to and comply with their moral dictates, assuming that they have an automatic right to steer our morality in their own chosen direction. If they think they’re ‘leading,’ most Australians aren't following.
The indications are that they're going the way of Kodak, now a small, wan shadow of its former dominant self. If the Anglican and Catholic churches were companies with voting shareholders (or even not-for-profits with voting members), the Boards and executives (archbishops and bishops) would have been, for overseeing such profound and continuing erosion of their brand franchises, replaced long ago.
Entrenched rather than learning
You’d think all this would be a warning message to archbishops and bishops to seek to understand their flocks and build bridges for mutual understanding and engagement; to demonstrate a bit of flexibility in recognising alternative and equally respectable moral codes that were not established in ancient and very different times. But no.
Their recent performances on both voluntary assisted dying and marriage equality law reform suggest otherwise.
The fact is that to rebuild their franchises, the churches need to reach out to their Occasionals and to their Notionals — those who identify with the denomination but rarely if ever attend services. But the bishops have been pleasing only (some of) their Regulars and Devouts. It's a classic and literal case of “preaching to the converted.”
Voluntary assisted dying
In the matter of voluntary assisted dying (VAD) law reform, there are presently VAD Bills before both the NSW and Victorian parliaments. Figure 3 shows Australian attitudes toward VAD by religious affiliation.
Figure 3: Australian religious affiliation and attitudes toward VAD Source: AES 2016
Opposition to VAD amongst most denominations is very small, and really only makes an appearance amongst minor Christian and non-Christian denominations. Just 10% of Catholics and 7% of Anglicans oppose VAD, 5% and 3% of them strongly.
Figure 4 shows the real story. Opposition to VAD amongst Rejecters, Socialisers, Notionals and Occasionals is almost non-existent, and support is in a huge majority (85% of Socialisers, 89% of Notionals and 78% of Occasionals). Opposition to VAD amongst religion Rejecters is less than 2%. That is, opposition to VAD is almost entirely religious, although religious opposers pretend their opposition is nothing to do with faith.
Figure 4: Australian religious identity (ARI-6) and attitudes toward VAD Source: AES 2016
Only amongst Regulars and Devouts does opposition to VAD make a real appearance. Yet even amongst Devouts, with the strongest opposition, it’s in the minority (47%).
And what have the bishops been doing? They’ve campaigned strongly against VAD, spreading misinformation. Take for example the Catholic Church’s latest version of its anti-euthanasia polemic ‘brochure’ (Figure 5).
Figure 5: The Catholic Church’s latest polemic brochure against VAD Source: Catholic diocese of Byron Bay
This amateur production reveals a superficial understanding of the issues and a penchant for hyperbole. Worse, it employs significant misinformation in order to create FUD (fear, uncertainty and doubt), as does an advertisement taken out by a number of bishops from various denominations, in Melbourne’s major daily newspaper (Figure 6).
Figure 6: The June 2017 bishops' anti-VAD print advertisement Source: Herald Sun
The bishops’ manoeuvres will only alienate their congregation’s least committed members, the Notionals and Occasionals — the very people they should be wooing back to the pews, and who are strongly supportive of VAD as a valid and respectable response to intolerable and unrelievable suffering at end of life.
Perhaps the bishops would find this suggestion unpalatable, too much like a sales pitch. If that’s the case, one can only point out that selling the claim of saving of souls is the very task of evangelism. One could ask, “is your God likely to approve heartily of the continued withering of Australian faith?”
Marriage equality
The second contemporary example is marriage equality (ME). Figure 7 shows Australian attitudes to ME by religious denomination.
Figure 7: Australian religious affiliation and attitudes toward ME Source: AES 2016. Note: There was no ‘neither/nor’ option in this survey question
A clear majority of Australians in all groups except minor Christian denominations support marriage equality. That includes 74% of Catholics, 63% of Anglicans and 60% of Uniting Church members.
Figure 8 shows attitudes toward marriage equality by religious identity.
Figure 8: Australian religious identity (ARI-6) and attitudes toward ME Source: AES 2016
Support of marriage equality is in a clear majority amongst Rejecters (88%), Socialisers (82%), Notionals (73%) and Occasionals (71%). Around half (49%) of Regulars also support marriage equality.
Only amongst Devouts is support for marriage equality in the minority, with a quarter (25%) supporting and three quarters (75%) opposing it.
And what have the bishops been doing? They’ve run a massive campaign against marriage equality law reform. Indeed, the Anglican Archbishop of Sydney, Glenn Davies, announced that the diocese had donated, from precious church funds, $1 million to the ‘No’ campaign.
The public was even more dismayed to discover the diocese had granted just $5,000 to dealing with entrenched domestic violence in its ranks, at the same time as allocating the $1 million to preventing the equal expression of love.1
Given that marriage equality is almost certain to be legalised in Australia either directly after this voter ‘poll’ or in the term of the next Parliament, that’s an extraordinary squandering of a vast charitable sum for no net result. Calls have been made for the diocese’s tax-exempt status to be reviewed.
The evidence is incontestable: opposition to VAD is almost completely religious, and opposition to ME is largely religious, despite protestations to the contrary.
Bishops’ conduct in relation to these reforms, which most Australians want, have been unhelpful by resisting Australia’s move into the 21st century — on the basis of ancient interpretations of scripture to which only a small minority of Australians subscribe.
The bishops' conduct has run strongly counter to the compassion and understanding they could have shown in order to engage the Notionals and Occasionals amongst their flocks; to halt the erosion of their religious capital, and to rebuild it.
These bishops most certainly don't represent the general views and beliefs of most Australians on VAD or ME. Rather, they give the appearance of administrators who are determined to preside over smaller and smaller congregations: a kind of “slow euthanasia.”
Blog by Neil FrancisPosted on Thursday 12th October 2017 at 1:50am
The latest religious right 'think tank' lobby group, the Institute for Civil Society.
I challenge the latest religious right commentators opposing Victoria’s Voluntary Assisted Dying Bill to skip the flip-flopping and engage constructively.
They’re at it again. This time it’s the religious right’s latest ‘think tank’ front group, the impressively-named Institute for Civil Society. Sounds grand, doesn’t it?
But if you look into their lot in life, it’s to protect ‘religious freedoms.’ By that, they mean the right to lawfully discriminate against others of whom they disapprove, while at the same time arguing that they not be discriminated against.
Mark Sneddon and Sharon Rodrick of the ‘Institute’ published an opinion piece in Fairfax Media today.
In it, they slam the Victorian Government’s Voluntary Assisted Dying Bill, which was introduced into the Parliament recently.
They level several criticisms at the Bill to say it's not 'safe'. But they could have advanced any criticism of the Bill to claim, as they do, that “the vulnerable will be at risk” — a logical fallacy as I’ve pointed out before. The "vulnerable will be at risk", by circular definition, if the Bill is printed in black ink (as it is) instead of purple, but they didn't complain about the colour of the ink.
The flip-flop
The point is, they flip-flop because they’re remarkably inconsistent in their position. At the same time as pointing out supposed flaws in the Voluntary Assisted Dying Bill, demanding a much higher standard of proof about a number of things, they completely fail in their opinion piece to even mention — let alone demand the same level of safeguards for — an already-legal and equivalent hypothetical risk for the “vulnerable.”
Equivalent hypothetical risk in operation for nearly 30 years
In Victoria, patients have an inalienable right to refuse any and all medical treatment. No reason need be given, even if the treatment is life-saving. The Medical Treatment Act 1998, currently in force, has several safeguards to protect against coercion or undue influence. In Section 5(1), one doctor and “another person” (who can be anybody) must be satisfied that:
“the patient has clearly expressed or indicated a decision”; and
“the patient’s decision is made voluntarily and without inducement or compulsion”; and
“the patient has been informed” about their condition and “has appeared to understand that information”; and
“the patient is of sound mind and has attained the age of 18 years.”
They’re all the legislated safeguards for the refusal of life-saving medical treatment.
And how many cases of undue influence have been prosecuted in Victoria over the nearly 30 years the Medical Treatment Act 1998 has been in effect? Precisely none. Not one.
So much for Messrs Sneddon and Rodrick’s avaricious relatives lurking at every bedside.
A new, equivalent hypothetical risk
The Medical Treatment Planning and Decisions Act 2016, which will come into force in March next year and which extinguishes the Medical Treatment Act 1998 at that time, also contains several similar safeguards for the refusal of life-saving medical treatment.
In witnessing an Advance Care Directive (Section 17), the two signatories, only one of whom must be a medical doctor, must certify that:
the person “appeared to have decision-making capacity” in relation to the documented decisions; and
the person “appeared to understand the nature and effect of each statement”; and
“the person appeared to freely and voluntarily sign the document”; and
“the person signed the document in the presence of the two witnesses”; and
“the witness is not an appointed medical treatment decision maker for the person.”*
In Section 52 of the Act, a health practitioner is forbidden to administer medical treatment if they are aware the patient has refused it, however (lawfully) refused.
This Act was passed in the term of the current Parliament: that is, by the same State MPs who are now considering the Voluntary Assisted Dying Bill.
There was no great fracas over the sensible safeguards spelled out in the new Medical Treatment Planning and Decisions Act. There was no onslaught of “crisis!” op-ed screeds published in newspapers. There were no countless hours of talking heads tut-tutting and painting doomsday scenarios.
It was passed by the Parliament and accepted by the people as striking the right balance.
No safeguards at all in many cases
And that’s it: the sum-total of safeguards to refuse life-saving medical treatment in Victoria. However, if the patient refuses medical treatment verbally, there are no mandated safeguards at all in either old or new Act, because the statutory safeguards apply only to refusal given in writing.
Yet despite all this, Messrs Sneddon and Rodrick rail against safeguards against coercion and elder abuse only in regard to the Voluntary Assisted Dying Bill, in which the safeguards are of a significantly higher calibre, with, for example, mandatory multiple doctor opinions, documentation trail, multiple requests, no go-ahead until approval by an external authority, notifications of numerous kinds, oversight by a specially-established panel, and so on.
It’s obvious what a flip-flop Messrs Sneddon and Rodrick’s demands are in respect of decisions that will foreseably result in death.
Another embarrassing flip-flop
Messrs Sneddon and Rodrick particularly also complain at length at the supposedly ‘lax’ definition of decision-making capacity in the Voluntary Assisted Dying Bill.
That’s a major and embarrassing flip-flop. Here’s why.
The section of the Voluntary Assisted Dying Bill that stipulates those requirements (Section 4) is the same section number 4 that governs the right to refuse of life-saving medical treatment in the Medical Treatment Planning and Decisions Act 2016. Only a few words have been changed to alter the context from refusal of treatment to consideration of assisted dying. Otherwise, the Sections are identical.
Messrs Sneddon and Rodrick don't point this out in their opinion piece. Indeed, I was unable to find online any evidence that they had published any complaint about the provisions when the Medical TreatmentPlanning and Decisions Act was in debate, nor since. If they have, I’d be happy for them to point it out.
Is it all a strategic ruse, anyhow?
It’s pertinent to ask if the objections are a ruse anyhow, because, as Andrew Denton has rightly pointed out, a key opponent strategy is not to give an outright “no” to assisted dying Bills, but to say only “not this Bill” and create an atmosphere of FUD (fear, uncertainty and doubt) so that it is defeated.
A typical ruse example
By way of example, I’ve published an account of how Victorian MP Daniel Mulino published outrageous misinformation about assisted dying. As a result, we had an extended conversation, during which he acknowledged that he had indeed published misinformation. At the end of the conversation I asked if he could support the Government’s Voluntary Assisted Dying Bill. (He’s a member of said Government.)
No, it’s too liberal, he said, pointing to Oregon’s Death With Dignity Act, now in force for nearly 20 years, as a more conservative approach. So I asked him if he would support a Bill like Oregon’s.
No, he said, there were still concerns about it.
By now you’ve spotted the merely incremental withdrawal of supposed possible support. So I asked him outright if there was any form of assisted dying Bill he could support.
The relevant word within a long discourse: No.
And there’s the answer that belies the political strategy. It doesn’t matter one whit what provisions are included in an assisted dying Bill, just criticize a bunch of provisions and create FUD to defeat it.
A direct challenge to Messrs Sneddon and Rodrick
If “doubters of this Bill” are genuine about permitting assisted dying in some defined circumstances, the duty is on them to define those circumstances and recommend wording to enact it.
And that’s the challenge I throw down directly to Messrs Sneddon and Rodrick. Don’t just bitch and gripe: define precisely what provisions and wording you think would be acceptable.
If you fail to stipulate what you deem acceptable, then your opposition to “this flawed Bill” is, like the supposedly ‘soft’ opposition of other campaigners in the negative, merely a ruse.
And that’s rather suggested by your deliberate use of the term “killing” for what most Australians believe to be an understandable and welcome release. But let’s give you the benefit of the doubt… for now.
Will you rise to the constructive challenge, or lurk in the shadows merely making snide remarks and flip-flopping?
----
* Section 62 of the Act also requires a doctor to notify the Public Advocate if “significant treatment” is refused — but only if it is refused by a substitute decision maker on behalf of the patient: not by the patient herself. And “significant treatment” is defined as treatments (not non-treatments) which are likely to have a serious impact on the patient (bodily intrusion, risk to life, side effects or distress). “Significant treatment” in the Act does not mean treatment whose refusal may result in death.
Blog by Neil FrancisPosted on Tuesday 10th October 2017 at 7:58am
The Parliament of Victoria is currently debating an assisted dying Bill.
As the Parliament of Victoria prepares to debate an assisted dying Bill, South Australian Catholic anti-assisted-dying lobbyist Mr Paul Russell is at it again. This time he's sent a missive to Victorian politicians shouting about, amongst other things, a crisis of assisted dying numbers in Washington state. He’s conveniently cherry-picked his arguments again.
Mr Russell wrote that in Washington state:
“deaths from lethal drugs prescribed under the Act have nearly quadrupled (376%) from 51 in 2010 to 192 in 2016.”
His latest claim extends his misinformation crown title.
Don’t get me wrong. He cites the correct raw data figures for Washington. But he packages them up handily with FUD (Fear, Uncertainty and Doubt) wrapping, all tied up with the most sinister bow he can muster.
I’ve criticised the use of uncontextualized raw data before, and I do so again.
The relevant facts
Washington state legalised assisted dying by ballot in 2008. The following year the law was put into practice, and 2010 was the first full year of its operation.
Here’s the rate of assisted deaths as a proportion of all deaths in Washington state for all the years on record. As you can see, the rate hasn’t even reached one half of one percent of all deaths in 2016.
2009
2010
2011
2012
2013
2014
2015
2016
0.07%
0.11%
0.14%
0.17%
0.23%
0.24%
0.30%
0.35%
Never ones to miss out on an opportunity to spread FUD, if it were just one case last year and two this year, assisted dying opponents would be shouting from the rooftops: “Crisis!! 100% increase!!”. But in reality, only a small minority use the law, yet thousands of patients and their families are given comfort by the option being avaialble even if they don't use it. That message was made loud and clear by Oregon Senator Ginny Burdick. Washington's Death With Dignity Act is modelled on Oregon's, and Oregon's Act has been in effect for twenty years.
A Catholic trifecta
Of course in his missive, Mr Russell, like his fellow Catholic whom I’ve also called out for misinformation, Prof. Margaret Somerville, avoids referring to Swiss data. And their fellow Catholic Mr Daniel Mulino, who furnished a minority report to the Victorian Parliament’s recommendations on end of life choices, a report I’ve also called out for stunning misinformation, fudges his numbers about Switzerland, referring to data from 1998 without further context.
Why do these lobbyists avoid or selectively refer to the Swiss situation? Because the actual data is an inconvenient truth to their FUD story-telling.
An inconvenient truth
Switzerland’s assisted dying law came into effect seventy-four years ago, in 1942. If just one person had used the law in 1942, using Mr Mulino’s favourite annual increase figure of 17.5%, that would equate to 110,338 people pursuing an assisted death in Switzerland in 2014.
I say 2014 because that’s the most recent year for which official Swiss Government assisted dying figures are available. And what was the actual figure in 2014? There were 742 cases of assisted dying amongst Swiss residents, and Dignitas reports that it assisted 198 foreign nationals. That’s a total of 940 assisted deaths.
Let’s add another 60 foreign-national assisted death cases from the much smaller Swiss society that provides accompaniment for foreigners. That makes around 1,000 cases in 2014, including all those who came from all over the world. And it’s less than one hundredth of the minimum rate the doomsayers predict by cherry-picking one statistic that suits their argument.
Swiss law has the fewest safeguards
The Swiss assisted dying law has none of the safeguards of the Washington law. By Mr Russell and Co’s reckoning, you’d think that the Swiss (and those who visit) would be dropping off like flies.
By way of further comparison, the doomsayer number of assisted deaths for 2014 (a minimum of 110,338 cases) is substantially greater than the total number of deaths in Switzerland that year: 63,938. It’s an obvious impossibility.
In 2014, the Swiss rate of assisted deaths including all the foreign nationals who came to use its law, was 1.5% of all deaths; and 1.2% for resident-only cases.
And the rate of assisted deaths in Luxembourg in 2014 (legalised in 2009), whose laws are much more liberal than Washington’s though stricter than Switzerland’s, was 0.17% of all deaths. It’s odd how the doomsayers don’t report Luxembourg data, either.
And what are these cases?
These are cases of people in extremis with no realistic prospect of relief or improvement, choosing a peaceful assisted death as a better option than being forced to prolong their torture, according to their own deeply-held beliefs, values and examined consciences.
Mr Russell believes they should be required to endure their torture. There is a point to it, he says: because it joins them “in some mysterious way to the sufferings of Christ”... whether others believe in Christ, or at least Mr Russell’s version of him, or not.
You won't find this degree of candour on his anti-assisted dying website, but you can find it at NewsWeekly, which is run by the National Civic Council (NCC), itself established by Australia's most famous and conservative lay Catholic, B. A. Santamaria. Mr Russell has been President of the NCC South Australian chapter.
It’s not the numbers, it’s the circumstances
To be clear, in no jurisdiction has its legislature enacted access to assisted dying on the basis of a numeric ceiling. They’ve enacted access on the basis of intolerable and unrelievable suffering. And to this day, those are the folks who may be granted access to an assisted death.
Conclusion
Again, Mr Russell (and colleagues) do themselves no favours by conspicuously cherry-picking the data they want to use, and wrapping it up in threatening garb to create FUD amongst politicians.
Blog by Neil FrancisPosted on Tuesday 19th September 2017 at 10:30pm
The Age reports on the three AMA dcotors' appearance at Spring Street
As reported in The Age, on Tuesday this week three AMA doctors fronted the Victorian Parliament to spread the word about their perceived horrors of an assisted dying law. Their arguments don’t hold water and politicians should see them for what they are: utter nonsense.
Doctors Stephen Parnis, Mukesh Haikerwal and Mark Yates say they will continue to lobby politicians.
With what?
Here is the ‘substance’ of their arguments — a sticky blomonge of the same old confected and discredited claims.
The vulnerable will be at risk
Dr Parnis said that such a law “puts the most frail and vulnerable in our community — the dying — at profound risk,” pointing to coercion, and patients not getting the medical care they need.
As I’ve explained before, the claim is flapdoodle — circular nonsense.
It’s a circular argument (a logical fallacy) because “the vulnerable” are by definition those “at risk” and vice versa. While the circularity makes the claim about assisted dying risks seem true, it's a false imputation.
By way of comparison, we could equally say that “the vulnerable will be at risk if we wear yellow socks on Wednesdays,” so we should outlaw that as well. Or anything else of which we disapprove and make our argument seem valid by attaching it to “the vulnerable being at risk.”
Let’s not talk about it
Dr Yates argued that the Parliament should not be pursing “divisive legislation.” That’s also a false argument because it's merely an appeal to emotion: avoiding legislating anything upon which there is any disagreement and discomfort. The consequence of this argument is to not legislate at all.
Patient trust in doctors
They also argued that assisted dying legislation would “change the doctor-patient relationship” — by which they mean “damage the relationship,” or they wouldn’t have mentioned it.
Again, as I have shown before, the empirical evidence from around the world is consistent with improved, not damaged, patient trust in doctors where assisted dying is legal.
The massive AMA flip-flop
But, as I’ve also pointed out before, the real telltale of the AMA doctors’ farcical representation to the Victorian Parliament is this: while opposing assisted dying legislation because patients might be pressured, subtly or otherwise, to choose death, the AMA officially endorses the right to refuse medical treatment, which includes life-saving treatment.
The hypothetical risk of patients being encouraged to refuse life-saving medical treatment is identical in kind to that of assisted dying. Yet in Victoria, the right to refuse is protected by just three statutory safeguards, while the assisted dying legislation is founded on no fewer than 68 safeguards.
So the AMA incoherently promotes one hypothetical pressure-to-die pathway with only three protections, while cruelly opposing a parallel path with an armada of protections. Let's award 10 out of 10 for the impressive flip-flop manoeuvre.
Conclusion
The AMA doctors’ claims are without merit and advancing them does no favours to their professional credibility.
Blog by Neil FrancisPosted on Thursday 14th September 2017 at 10:20pm
Another Catholic 'academic' spreads more misinformation. Photo: donaldytong
It’s very disappointing that Catholic theologian Dr Joel Hodge’s recent editorial in Fairfax media about assisted dying law reform contained misinformation: the same old tired and discredited story trotted out as though it's true. Dr Hodge also repeated an old and curiously one-sided (Catholic) examination of the hypothetical slippery slope.
Unhappily, the kind of misinformation that Dr Hodge advances muddies the waters and cruelly stands in the way of legislative action, which most Australians want.
An impeccable national survey conducted by scholars at Australian National University last year found 77% of Australians in favour of assisted dying law reform. Strong support (43%) outweighed strong opposition (4%) by more than ten to one. In the two states whose Parliaments are currently considering reform, NSW and Victoria, support stands at 75% and 79% respectively.
Non-religious support is 91%, and it’s high amongst Catholics (74%) and Anglicans (79%) as well. Bishops are jarringly out of step with the views of their flocks. And across the political spectrum, 87% of Greens, 80% of Labor, 77% of Coalition and 69% of minor party voters also want reform.
The electorate’s desires couldn’t be clearer. But politicians — who have little time to fact-check what they’re told — are fed the kind of misinformation Dr Hodge advances.
The false 'non-voluntary euthanasia slippery slope' argument
He quotes details from a medical journal article by Dr José Pereira, a Canadian Catholic physician. Like others who cite this article, Dr Hodge fails to mention that it was thoroughly debunked in a surgical deconstruction by expert scholars. They found Pereira’s claims variously unsupported by any evidence, unsupported by the sources he cited, or false, concluding that the article was “smoke and mirrors.”
Like other Catholics, Dr Hodge relies heavily on a thoroughly debunked journal article by Catholic Canadian doctor, José Pereira.A significant source of smoke, which Dr Hodge fans from this debunked article, is the claim regarding “900 Dutch deaths hastened without explicit request”: that is, non-voluntary euthanasia or NVE. Such figures are cited as ‘proof’ of the hypothetical slippery slope from legalised voluntary euthanasia to NVE.
Other opponents of assisted dying variously put the figure at 500 or 1,000. For the sake of argument, let’s say the 900 figure is equivalent to 1,000. Both the 500 and 1,000 figures, also repeatedly promoted by Catholic ethicist Professor Margaret Somerville and others, have been true. But here’s the thing.
What they don’t mention is that the 1,000 rate is from the 1990s when Dutch assisted dying was conducted under a general regulatory framework. In 2002 the Dutch euthanasia Act came into effect. Amongst the Act's many details was the establishment of a Commission which examines every reported case of assistance.
Since then, the Dutch NVE rate has dropped to 500, and even further. It has stayed low and is now similar to the NVE rate in the United Kingdom, the world’s gold standard for palliative care, and where assisted dying remains illegal.
There was a significant drop in the NVE rate in Belgium, too, after its euthanasia Act came into effect, also in 2002.
It is absolutely unconscionable that yet another Catholic commentator has trotted out the same old lie as though it's true. Dr Hodge is an academic and it is incumbent on him to check the facts before sounding off.By cherry-picking a single figure, opponents argue the opposite of the facts, implying or even directly claiming that NVE rates are caused by or have risen as a result of legalised assisted dying. I’ve comprehensively exposed this nonsense before, yet it comes up repeatedly.
It’s similar to other lines of Catholic argument against assisted dying, like the claim that Dutch elderly supposedly travel to Germany for healthcare because they fear being euthanised by their Dutch doctors — an outrageous falsehood. There’s also the faintly desperate claim that Dr Els Borst, the architect of the Dutch euthanasia Act, later regretted her reform — a fake claim she’s firmly corrected.
Consider too a Catholic bishop’s claim, without reservation and in formal evidence before an official Parliamentary inquiry, that Oregon’s general suicide rate was very low prior to its assisted dying Act but very high afterwards — contrary to the facts. Or a report cherry-picking just half a sentence from a journal paper to claim that a significant proportion of assisted-death patients in Oregon had symptoms of depression, when the other half of the verysame sentence clearly stated that none of them had.
As Professors Griffiths, Weyers and Adams wrote in 2008, “imprecision, exaggeration, suggestion and innuendo, misinterpretation and misrepresentation [and worse] took the place of careful analysis.” Sadly, the same still seems true today.
Major Catholic flip-flop on choosing death
Now let’s turn our attention to the core of Dr Hodge’s thesis. His plea for “the vulnerable” leads his argument and is heavily egged throughout the polemical pudding.
A comparison is moot: Australians have the right to refuse any unwanted medical treatment, even if it’s life-saving.
In my home state of Victoria, this right to refuse is enshrined in statute. The statute contains just three ‘safeguards’ for checking a refusal, and those only apply if the refusal is formally documented in writing but not if it’s only oral.
As I’ve explained in detail before, the consequence is that a person can refuse life-saving medical treatment with few if any checks and balances. In theory, just as Dr Hodge argues in regard to assisted dying, the person might feel pressured by greedy relatives, resource-poor doctors or others, to so refuse.
In this case, where is the Catholic call for protections? Where is the moral outrage on behalf of ‘vulnerable patients’? There is none. In fact, the Catholic Church’s call is quite the opposite. In a directive to all Catholic healthcare institutions in the USA, the Conference of Catholic Bishops make the Church’s position abundantly clear. They direct that there is no obligation for patients to use “disproportionate means of preserving life.”
The Catholic church's rhetoric against assisted dying is a major flip-flop when compared to its cosy attitude towards refusal of life-saving medical treatment: both might result in hypothetical pressure to choose death, yet only assisted dying has adequate safeguards.They define disproportionate means as “…those that in the patient’s judgement do not offer a reasonable hope of benefit or entail an excessive burden, or impose excessive expense on the family or the community.”
So, under two identical hypothetical possibilities of inappropriate persuasion to choose death, Dr Hodge’s argument bristles against an assisted dying reform containing — as he acknowledges — no fewer than 68 safeguards, while his Church argues that patients may refuse life-saving medical treatment if the patient feels it’s “hopeless,” entails “excessive burden” or imposes “excessive expense” on others, with hardly any, or no statutory safeguards at all.
The incoherence, and repetition of misinformation, is indefensible. Civil debate on such an important matter deserves better.
Blog by Neil FrancisPosted on Sunday 6th August 2017 at 2:31am
The terminally ill are not choosing between life and death, but between two ways of dying, according to their own beliefs and conscience. Photo: Andrew Drummond/AAP
In Monday’s Herald Sun, Victorian Archbishops Philip Freier and Denis Hart, and Bishops Ezekiel, Suriel, Lester Briebbenow, Bosco Puthur and Peter Stasiuk published a half-page advertisement admonishing the Victorian government for its initiative to legalise assisted dying for the terminally ill, an ad similar to the one published by religious figures in 2008.
I have no quarrel with individuals of faith regarding their own private beliefs. However, the bishops’ attempt at public “leadership” through the advertisement is deserving of redress for its multiple fallacies.
The ‘abandonment’ fallacy
The bishops claimed that assisted dying “represents the abandonment of those who are in greatest need of our care and support”. On the contrary: to ignore the deeply-held beliefs and rigorously-tested wishes of people at the end of life is to abandon their values and critical faculties in favour of the bishops’ own religious dogma.
The ‘competition’ fallacy
The bishops demand there should be more funding for healthcare rather than assisted dying, fallaciously pitting one option against the other. The Victorian government is indeed increasing funding for palliative care. It’s also aiming to provide lawful assisted dying for when even the best palliative care can’t help – which Palliative Care Australia has acknowledged – giving lie to the faux competition.
The evidential fallacy
Contrary to the bishops’ false presumption that legalised assisted dying will decrease trust in “the treatment and quality of care” from doctors, scientific studies into attitude change show that more people trust doctors when assisted dying is legal. Patients can then talk openly about options, even if they decide against assisted death. The bishops have abandoned facts in favour of religious assumptions.
The equivalence fallacy
The bishops refer to assisted dying as “government endorsed suicide”. They fallaciously equate a reasoned, tested and accompanied decision for a peaceful assisted death in the face of a terminal illness, with the impulsive, violent, isolated and regrettable suicide of individuals (many of whom have mental health and substance abuse issues) who are failing to cope with problems that can be addressed.
However, while the latter are choosing between life and death, the terminally ill are choosing not between life and death, but between two different ways of dying, according to their own beliefs and conscience. Rigorous 2016 research from Australian National University shows that the vast majority (79%) of Victorians support assisted dying choice for the terminally ill (with just 8% opposed), clearly distinguishing it from general suicide.
Shame on the bishops for disrespectfully equating the two.
The inconsistency fallacy
They also argue that assisted dying ought to remain prohibited because within healthcare, “mistakes happen and the vulnerable are exploited,” and “that in spite of our best efforts, our justice system could never guarantee” no one would die by mistake or false evidence. However, as I’ve pointed out before, an identical hypothetical problem exists under the refusal of life-saving medical treatment, a statutory right that Victorians have enjoyed for nearly 30 years. The statute has only three “safeguard” requirements, yet even those only apply if the refusal is formally documented, but not if it’s verbal.
Further, the United States Conference of Catholic Bishops directs that patients may refuse treatment if it imposes “excessive expense on the family or community,” yet makes no mention of the hypothetical “vulnerability” of the patient to be persuaded so, nor directs any requirements to assess the veracity of the refusal.
In stark contrast, the Victorian proposal for assisted dying legislation contains more than 60 safeguards and oversights.
The bishops are at risk of ridicule for such a gargantuan flip-flop: supporting the refusal of life-saving treatment with little or no oversight, while vocally opposing assisted dying legislation that mandates an armada of protections.
The not-so-hidden agenda
The bishops’ methods are rather unsubtle – hoping that these arguments, erroneous but carefully crafted to avoid any religious connotations, will be accepted as non-religious. Yet religion is writ large across their plea: as signatories to the letter they are all clerics employed directly and centrally in the promotion of their religions.
The authority fallacy
They might also rely on their religious status to convey gravity and authority to their pleas. Yet as people paid to do a job, like anyone else, their titles grant them no special privileges in lecturing Victorians about how they should die in the face of a terminal illness.
According to the 2016 census, just 23% of Victorians identified as Catholic, 9% as Anglican, 0.5% as Lutheran, and the other bishops’ signatory denominations so small as to not appear separately in the government’s statistics. Combined, the bishops’ faiths represent around 33% of the Victorian population, while 32% of Victorians identify with no faith at all. Surely the bishops are not arguing that they’re speaking for these other Victorians, too?
But the bishops don’t represent the views of their own flocks, either. According to the 2016 ANU study, 89% of non-religious Victorians support assisted dying law reform, as do 78% of Victorian Catholics and Anglicans. Indeed, opposition to assisted dying exists mostly among those who attend religious services once a week or more often – that is, those who are frequently exposed institutional religious messages of opposition – yet who comprise just 12% of Australians and 11% of Victorians.
Minding their own flocks
Australians are abandoning religion in droves. For example, when Freier ascended to the top job of Anglican Primate of Australia in 2006, some 19% of Australians identified as Anglican (2006 census). A decade later under his leadership, the 2016 census showed a drop of about a third to just 13%, and in Victoria, his home territory, to just 9%.
Hart’s Catholic church has experienced a drop in affiliation too, and it’s likely to continue and accelerate as Australians react with shock and disgust to the extent of child sexual abuse that the royal commission has exposed from under his organisation’s “pastoral umbrella”.
In conclusion, rather than bishops lecturing the government and Victorians with fallacious and faintly desperate arguments about the choices they shouldn’t have at the end of life, attending to their own flocks may be more useful Christian leadership.
May their God go with them in that endeavour.
This article was originally published in The Guardian.
To add insult to injury, it flip-flops on its stance.
Never mind that the argument is contradicted by evidence
The Church’s favourite argument — already contradicted by scholarly analysis that curiously seems to be of no interest to the Church — is this: if people are given the choice of assisted dying, they will feel compelled to choose it, coerced by doctors, greedy relatives or others; subtly or otherwise.
No matter that health care workers routinely report that relatives usually try and persuade their dying loved one to endure yet another invasive and burdensome treatment; not dissuade them from it.
The flip-flop
If the Catholic Church were indeed genuinely concerned about coercion of ‘the vulnerable,’ then it would equally oppose the right to refuse medical treatment, particularly if the treatment were life-prolonging. But it doesn’t.
If granny might die as a result of refusing a particular medical intervention, then a doctor might persuade her to refuse in order to conserve medical resources. Or greedy relatives might persuade her so that they are relieved of the burden and expense of looking after her and gain earlier access to her estate.
As eminent legal scholar Gerald Dworkin has argued,1 if there’s a theoretical ‘slippery slope’ for assisted dying, it’s the same for the refusal of life-preserving medical treatment.
To hold different positions under the same risks is to flip-flop. That’s especially so when there are numerous safeguards built into assisted dying statutes, but currently few or none for the right to refuse life-preserving medical treatment.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
Local experience confirms risk is theoretical
In my home state of Victoria, where the right to refuse any unwanted medical treatment has been enshrined in statute for nearly three decades (the Medical Treatment Act 1988), how many prosecutions have there been under the Act’s provisions against inappropriate persuasion?
Precisely none. Not a single case. So much for the theory.
It all serves to highlight that the Catholic Church’s only real argument is that it believes that it’s morally wrong to deliberately hasten death. However, it avoids this argument because as a religious tenet, it doesn’t appeal to the masses.
Catholic directives
The Church’s flip-flop about ‘the vulnerable’ is not a one-off accident. Take for example the ‘Ethical and Religious Directives for Catholic Health Care Services’ published by the United States Conference of Catholic Bishops.2
The Bishops ‘direct’ that there is no obligation on patients to use disproportionate means of preserving life. They state that disproportionate means are:
“…those that in the patient’s judgement do not offer a reasonable hope of benefit or entail an excessive burden, or impose excessive expense on the family or the community.”
The Bishops further ‘direct’ that:
“The free and informed judgment made by a competent adult patient concerning the use or withdrawal of life-sustaining procedures should always be respected and normally complied with, unless it is contrary to Catholic moral teaching.”
Setting aside the Church’s hubris of dishonouring the patient’s choice if the Church disagrees, it would be theoretically easy for someone to persuade the patient that hope was not reasonable, that the burden would be too great, or that the cost to the family or society would be too high.
Suffering for our God’s (your own) good
On the next page, the Bishops expressly ‘direct’ that:
“Patients experiencing suffering that cannot be alleviated should be helped to appreciate the Christian understanding of redemptive suffering.”
That’s unqualified. So, if you’re atheist, agnostic, Jewish, Hindu, Muslim or even a Christian who believes assisted dying can be appropriate, as a patient in their institutions you are to be persuaded that suffering against your beliefs and wishes is ‘redemptive’ in the eyes of the Vatican’s version of a God.
In Australia in 2009, for the Office for Family and Life in the Catholic archdiocese of Adelaide, Mr Paul Russell argued in News Weekly that “there is a point to suffering” because:
“It’s about the profound connection that each and every life has to the incarnate God … We know that the sufferings we endure well are joined in some mysterious way to the sufferings of Christ.”
Pity any poor soul who doesn’t share Mr Russell’s views. Curiously, there is no mention of this underpinning belief in his anti-assisted dying blog, “HOPE.”
Invalid argument in any case
The Church’s argument that ‘the vulnerable’ will be ‘at risk’ from assisted dying laws — for example in the Victorian Bishops’ recent pastoral letter to the Catholics of Victoria opposing the upcoming assisted dying parliamentary Bill — is itself fundamentally invalid.
That’s because, as I’ve previously explained, it’s a circular argument: a logical fallacy.
A circular argument: We must ban yellow socks on Wednesdays or the 'vulnerable' will be 'at risk'.‘The vulnerable,’ by definition are those ‘at risk,’ and will still be so if we wear yellow socks on Wednesdays. Therefore, we should ban such bright footwear midweek — and anything else we happen to oppose — on the same basis.
Might anyone suggest that “we should ban religion because the vulnerable will be at risk of succumbing to extreme religious views”?
Will the Church change its mind?
The Catholic Church does change its mind from time to time, though its reforms are glacially slow.
Take, for example, its theory of limbo, a place on the doorstep of hell where, the Church claimed, babies go if they die before they’re baptised: that they’d be prevented from entering heaven. It would be hard to imagine a crueller worry to put into the heads of uneducated new parents.
But in 2007, after centuries of confidently promoting the theory, the Catholic Church decided that it was wrong and buried it.
Will it change its mind on assisted dying? Maybe, but don’t hold your breath.
Conclusion
The Catholic Church, reeling from its extensive failure to protect our most vulnerable — children — and notwithstanding some good individuals within, still presumes to morally lecture the rest of us with the logical fallacy of how ‘risky’ assisted dying legislation is supposed to be to ‘the vulnerable,’ while flip-flopping in support of refusing life-saving medical treatment under the same theoretical risk.
The Bishops’ rhetoric amply exposes their confected crisis against assisted dying as nothing but religious doctrine draped in faux secular garb… in reality a sheep in wolves’ clothing.
References
Dworkin, G, Frey, RG & Bok, S 1998, Euthanasia and physician-assisted suicide, Cambridge University Press, Cambridge, New York. pp.66ff
Blog by Neil FrancisPosted on Wednesday 21st June 2017 at 3:14am
More Dutch evidence contradicts Margaret Somerville's 'suicide contagion' theory
I’ve previously published an extensive analysis of how Professor Margaret Somerville, of the Catholic Notre Dame University of Australia, cherry-picked her way through select data that seemed to be (but wasn’t) consistent with her ‘contagion’ theory from assisted dying to the general suicide rate. I provided ample evidence from lawful jurisdictions that comprehensively contradicts her claim. I also published the summary in ABC Religion & Ethics.
Yet Somerville still says despite extensive real-world experience to the contrary, that “I believe that my [suicide contagion] statement will prove to be correct.”
She and her Catholic colleagues still hold onto several tenuous threads of information that might — just might — appear consistent with her theory, despite the truckloads of evidence to the contrary.
One of those tenuous threads is that the general suicide rate in the Netherlands has increased from 2008, around the same time that use of the Dutch euthanasia law also increased. (The general suicide rate previously fell as assisted dying rates increased.)
I reported official Dutch government statistics and expert financial reports to show that the unemployment rate explains most (80%) of the variation in the Dutch general suicide rate since 1960, and that the Netherlands was particularly hard-hit by the global financial crisis from 2008 — whereas neighbouring Belgium wasn’t and its suicide rate dropped as assisted dying numbers increased. Unemployment in hard times is a known significant risk factor for suicide.
Now, a detailed and peer-reviewed analysis of Dutch data recently published in the Netherlands Journal of Medicine throws more mud in the face of Somerville’s theory.1
The research looked at the Dutch assisted death and general suicide rates from 2002 through 2014, separately for each of the five Euthanasia Commission reporting regions.
Headline results of the averages for 2002–14 are shown in Figure 1.
Figure 1: The average assisted death rate (and suicide rate) as a percent of all deaths by region, 2002-14 Source: Koopman & Putter 2016
As you can see, Region 3, which includes Amsterdam, had by far the greatest assisted death rate (3.4%), compared with the other four regions (1.7% – 2.0%). Yet Region 3’s suicide rate at 1.2% was the same as Region 5 which had only half the assisted death rate of Region 3 (1.7% vs 3.4%). (The authors, unusually, expressed suicides as a percentage of all deaths rather than per 100k population.)
The results are the opposite of Somerville’s theory which says that Region 3’s general suicide rate should be much higher than (not the same as) Region 5’s.
Those figures are the average for 2002–14. It’s possible that the picture is a little different for the more recent years in which the assisted dying rate is higher.
To answer that question, I’ve retrieved official Dutch Government data and calculated the assisted dying rates and general suicide rates for 2014 alone, the most recent year for which all the data is available. I’ve also calculated the general suicide rate per 100,000 population, the more usual way of reporting and comparing suicide statistics. The results are shown in Figure 2.
Figure 2: The Dutch assisted death rate and general suicide rate by region for 2014 Sources: Euthanasia Commission annual reports, Dutch Government statistics
While region 1 (the far north) has the lowest assisted death rate (3.2% of all deaths), it has by far the highest general suicide rate (13.6 per 100k population).
The latest Dutch regional data shows the opposite of Margaret Somerville’s ‘suicide contagion’ theory, adding to the already extensive evidence against it.Conversely, region 3 (which includes Amsterdam) has by a very large factor the highest assisted dying rate (6.0% of all deaths), yet it has the second-lowest general suicide rate (10.3 per 100k population).
This latest empirical evidence is consistent with other extensive evidence I’ve published showing an inverse — or no — relationship between assisted dying rates and general suicide rates.
The question is whether Margaret Somerville and her Catholic friends will pay the slightest attention, or continue to rely on invalid, cherry-picked morsels of data that they think support their theory, but don’t.
References
Koopman, JJE & Putter, H 2016, 'Regional variation in the practice of euthanasia and physician-assisted suicide in the Netherlands', Netherlands Journal of Medicine, 74(9), pp. 387-394.
Blog by Neil FrancisPosted on Tuesday 13th June 2017 at 2:38am
The Age reports a 'gloves off' campaign of misinformation
Both the Herald Sun and The Age reported last week that religious anti-assisted dying crusaders are running a 'gloves off' campaign in Victoria.
Religious forces are gathering once again to attempt to thwart the views of the great majority of Victorians in favour of assisted dying law reform.
Matt Johnston in the Herald Sun quoted Paul Russell, a long-term figure in Catholic circles, and Greek Orthodox Bishop Ezekiel, in statements against assisted dying.
Farrah Thomazin in The Age quoted religious stalwarts Margaret Tighe of Right To Life, and the Australian Christian Lobby, in further statements against assisted dying.
The crux of the story is that 'pollsters' claim to have run a survey in Victoria. They refuse to be identified. They refuse to publish their methodology. And they refuse to publish all their results. Enough said.
They cherry-pick an item from their supposed poll to claim that 33% of Victorians who oppose assisted dying will change their vote against a supporting politician at the next election. They neglect to mention that only a tiny minority of Victorians actually oppose assisted dying. Their analysis is astonishingly superficial, even assuming they ran a proper, robust poll and didn't manufacture the numbers themselves.
They then use this tidbit of 'data' to put the fear of electoral defeat into politicians who will soon to face an assisted dying Bill in the Victorian Parliament.
What rubbish. Assisted dying (AD) opponents seem to be utterly shameless in misrepresenting and distorting cherry-picked data to push their religious agenda — which they pretend isn't religious.
The real situation in respect of AD is the exact opposite of their claims as I show in a proper, robust analysis of legitimate data, demonstrating that:
A massive 78.9% of Victorians support AD, with only a tiny 8.1% opposed. Strong supporters outnumber strong opponents by more than ten to one.
Significantly more supporters of AD believe that law reform is personally important, than opponents believe the status quo (no law) is personally important.
At a general election, far more Victorian voters will punish Members who oppose the AD Bill than will punish Members who support it (3.5 to 1 overall, 2.4 to 1 for the Liberal/National Coalition and 6.6 to 1 for Labor).
The co-sponsors of Victoria’s 2008 AD Bill were returned with greatly increased majorities (including relative to their party’s overall performance) despite campaigns against them by anti-AD crusaders.
So that Victorian politicians are not misled, I have forwarded my report to the Victorian Government's Cabinet and other selected members of Parliament.
The only way in which this campaign could be called 'gloves-off' is that opponents, lurking around with their shadowy misinformation, don't want to get bullshit on their mittens. Hands seem to be much easier to wash. And hide.

 Figure 1: Australian religious affiliation by census year
Figure 1: Australian religious affiliation by census year") Figure 2: Australian denominations and Australian religious identity (ARI-6)
Figure 2: Australian denominations and Australian religious identity (ARI-6) Figure 3: Australian religious affiliation and attitudes toward VAD
Figure 3: Australian religious affiliation and attitudes toward VAD and attitudes toward voluntary assisted dying") Figure 4: Australian religious identity (ARI-6) and attitudes toward VAD
Figure 4: Australian religious identity (ARI-6) and attitudes toward VAD Figure 5: The Catholic Church’s latest polemic brochure against VAD
Figure 5: The Catholic Church’s latest polemic brochure against VAD Figure 6: The June 2017 bishops' anti-VAD print advertisement
Figure 6: The June 2017 bishops' anti-VAD print advertisement Figure 7: Australian religious affiliation and attitudes toward ME
Figure 7: Australian religious affiliation and attitudes toward ME Figure 8: Australian religious identity (ARI-6) and attitudes toward ME
Figure 8: Australian religious identity (ARI-6) and attitudes toward ME





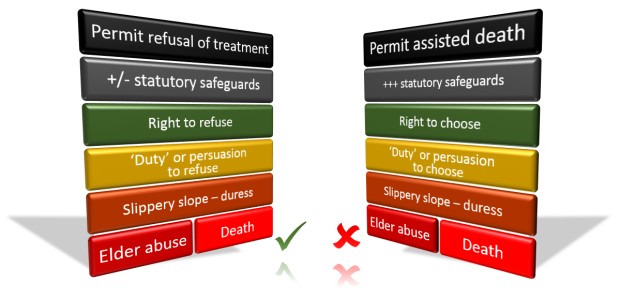 The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
 Figure 1: The average assisted death rate (and suicide rate) as a percent of all deaths by region, 2002-14
Figure 1: The average assisted death rate (and suicide rate) as a percent of all deaths by region, 2002-14 Figure 2: The Dutch assisted death rate and general suicide rate by region for 2014
Figure 2: The Dutch assisted death rate and general suicide rate by region for 2014