To represent a thing or situation as considerably more sinister or dangerous than it is when assessed objectively using evidence and balanced evaluation.
Blog by Neil FrancisPosted on Saturday 24th September 2016 at 11:31pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
Against current moves to legalise assisted dying, Australian Catholic Father John George invokes Nazi Germany, resorts to ad hominem attacks to dismiss those who disagree with him, and demands that the Pope’s edicts are binding on everyone regardless of their own faith or world view.
On 24th September 2016, Journalists Greg Brown and Rick Morton published an article in The Australian, Victorian coroner credited with turning tide on euthanasia, summarising recent Australian moves to legalise assisted dying choice.
Catholic Father John George commented on the article online, quoting four sections of the Catholic Church’s catechism that prohibit assisted dying (sections 2276–9).
Pushback
Other readers of The Australian remarked that they respected his view for himself but they had no interest in the Pope’s views given the readers were not Catholic. In fact, repeated polls in Australia have shown that even the great majority of Catholics (three out of four) do not agree with the Vatican on the matter of assisted dying, a matter which Fr George dismisses merely as ‘fickle votes and polls.’
I would remind Fr George that these are not fickle: Australian public opinion in favour of assisted dying choice has been consistently in the majority for now more than four decades.
Fr George further quoted Catholic sources, for example the LJ Goody Bioethics Centre in Perth, Australia, which he failed to mention is, literally, an agency of the Catholic Archdiocese of Perth. He also selectively quoted Palliative Care Australia, failing to mention that they have acknowledged that not all pain and suffering can be eliminated at the end of life, even with the best palliative care.
Ad hominem attack
In response to a rising tide of objections to his musings, including from Mr Ian Wood, a fellow Christian and co-founder of Christians for Voluntary Euthanasia Choice, Fr George resorted to the ad hominem attack: to attack the person (or persons) rather than the arguments. He said:
“The pro euthanasia claque here make professional Nazi propaganda expert Goebbels look like a 5th rate amateur.” — Father John George.
For anyone in the dark, a claque is a group of sycophants hired to applaud a performer or public speaker. How rude. Fr George seems to have neglected to reflect that it is he who is hired to promote the performance of the Vatican. I applaud his right to do so, and I do not compare him to a treacherous propagandist in a murderous wartime regime in order to dismiss his arguments: I address the arguments themselves.
Nazi Germany
Fr George makes repeated mentions of Nazi Germany as a core reason to deny assisted dying choice.
In contrast, several years ago I was chatting at a conference with the pleasant and engaging Peter McArdle, then Research Director of the Australian Catholic Bishop’s Conference. He volunteered that he very much disliked the “Nazi Germany” argument so often used in religious circles, and wished it would stop because in so doing it meant they’d already lost the debate.
I agree. It’s a lazy and indefensible argument: that rational people in a functioning democracy must be denied choice for themselves on the basis of what some murderous regime did against others at the point of a gun.
Indeed, to rely on such a standard would be to equally argue against the right to religious practice, because the Catholic Church, through its inquisition practices (medieval C12th, papal C13th, Spanish C15th, Roman and Portuguese C16th) relied on torture and resulted in confiscation of property and at least tens (if not hundreds) of thousands of executions for witchcraft and heresy.
Ultimate hubris
But the real crux is that Fr George then unequivocally demands that:
“Principles elaborated by the pope are universally applicable.” — Father John George.
This ultimate hubris reveals a profound lack of self-reflection, both personally and organisationally. Even entertaining for a moment the premise that one individual (or even organisation) can tell everyone on the planet how they must live their lives, how would we choose that person or organisation? Why is it less valid for the head of any other branch of Christianity, of Judaism, Islam, Hinduism, Buddhism (or any other religion) or an agnostic (which I am) or an atheist, to set such rules for everyone, overriding other deeply-held beliefs and values?
A keener example of ‘blinded by faith’ would be hard to find.
Conclusion
I argue that Fr John George displays some of the gravest hubris of some members of the Catholic church. I respect and applaud his world views for himself and those who wish to subscribe. But using canonincal arguments (that is, religious arguments demanded as universally true by virtue of the supposed authority that dispensed them) is probably a major contributor to the current flight of people away from organised religion.
More happily, such an attitude is also contributing to accelerating the legalisation of assisted dying choice because folks can see these arguments for what they are. For that I doff my hat to Fr George.
Blog by Neil FrancisPosted on Sunday 26th June 2016 at 2:05am
Schadenberg and Russell falsely call the Oregon Medical Association the "assisted suicide lobby" in contradiction of the facts.
Last week, Alex Schadenberg wrote—and Paul Russell republished—another nonsense article, this time about medical associations going neutral on assisted dying. They opine that there is no such thing as neutrality. And start out by getting their facts wrong... again.
Got the facts wrong yet again, lads
Messers Schadenberg and Russell claim that the Oregon Medical association is an "assisted suicide lobby" group. Had they bothered to check the rudimentary facts before sounding off, they would have known that the Oregon Medical Association remains neutral toward assisted dying. It reconfirmed its neutral stance as recently as early this month. It does not hold a 'supportive' stance.
How did Schadenberg and Russell come to their conclusion?
American Medical Association AGM
They refer to a motion that the Oregon Medical Association put to the recent annual general meeting of the American Medical Association. The motion sought to establish a process by which the American Medical Association would consult in order to re-evaluate its opposed stance to assisted dying, given that assisted dying is legal in a number of USA States and there are already many doctors who in good conscience provide assistance to die to qualifying patients.
Heavy-handed partisanship
In their usual style of heavy-handed partisanship, Schadenberg and Russell describe the Oregon motion as the "assisted suicide lobby" applying "pressure" to the American Medical Association.
They fail to level the same criticism at another group, the Louisiana Medical Society who put another motion to the meeting. The Louisiana motion sought to expressly confirm and entrench the American Medical Association's currently opposed stance. Schadenberg and Russell fail to criticize the Louisiana motion as "pressure," despite the fact that Oregon's motion was for open consultation, while Louisiana's was for a closed position.
Good sense prevails
In fact, they don't mention the Louisiana motion at all. Why? Because wiser heads prevailed at the national conference. The Louisiana motion was defeated and the Oregon motion was passed as I reported last week.
Desperate hyperbole
Schadenberg and Russell then desperately argue that you can only support or oppose assisted dying. There is no neutral, they say.
In the language of 'influence' we call this rhetoric "the sucker's choice." You put up just two options and demand folks pick one or the other.
"You're either for us or agin us!"
No other options, no nuances, no consideration of different options for different folks. Hardly the kind of stuff that would pass even a junior high school debate.
Back to the real world
Of course it's possible to be neutral.
Individually, a doctor may be personally opposed to assisted dying, but appreciate that another doctor, having equally examined their conscience, may support choice. Thus, the first doctor opposes for themselves but remains neutral to the position of other doctors. Indeed, an individual doctor may neither support nor oppose choice.
Collectively, it makes sense for a professional medical body to hold a neutral stance. How can it justify respecting the deeply-held beliefs and values of some of its members at the same time as explicitly disrespecting other members' views that are as closely examined and deeply held?
Conclusion
The best that opponents running the global charge against assisted dying can do is to first get their facts wrong (again), develop their false assumptions into shrill hyperbole, and then try to press the false dichotomy of a "suckers choice" into doing some heavy lifting: an exercise that falls flat on its face.
The evidence is crystal clear: they provide no real argument at all.
Blog by Neil FrancisPosted on Sunday 8th May 2016 at 9:48pm
Jeanne Smits' completely false statement in LifeSiteNews
Well it didn't take long. Recently I posted a fact-based report card on Dutch euthanasia practice, based on the actual data from the 2015 annual report (and all the earlier reports) of the Dutch Euthanasia Commission. Now, just a few days later, conservative religious opponents have begun publishing completely untrue statements about Dutch euthanasia practice.
Catholic blog LifeSiteNews' 'Paris correspondent' Jeanne Smits has bolted out of the misinformation blocks, assertively and categorically stating in respect of the small increase in number of euthanasia cases from 2014 to 2015, that:
"The rise is mainly due to the increase of euthanasia for demented, elderly people as well as psychiatric patients, two categories that raise even more questions than 'ordinary' euthanasia for untreatable physical pain."
Smits goes on to correctly report that dementia was an underlying factor in 109 of the cases in 2015 (against 81 in 2014) and psychiatric disorders in 56 patients (against 41 in 2014).
The total number of euthanasia cases increased from 5306 in 2014 to 5516 in 2015, an increase of 210 cases. The increase in dementia cases was 28 and in psychiatric disorders was 15. Therefore, underlying dementia accounted for 13% of the increase, and psychiatric disorders 7% of the increase.
Cherry-picking
Smits has cherry-picked just the dementia and psychiatric illness figures and presented them in a way that supports her story arc, painting a bleak picture.
But by no stretch of the imagination does dementia and psychiatric illness account "mainly" for the increase as she categorically states.
What didn't Smits report at all? Cancer: the Netherlands' leading cause of death. In 2015, cancer was the underlying condition in 4000 euthanasia cases, against 3888 in 2014, a rise of 112 cases or 53% of the increase. That compares with dementia at 13% and psychiatric illness at 7% (20% combined), which Smits selectively critiques as a 'sharp rise'.
In no way is Smits' statement true.
No, let's be frank: it's an outright lie. Cancer was the major underlying condition accounting for more than half of the small increase (4%) of cases in 2015.
More evidence refutes the claim
Comparing one years' data with just the preceding years' data can be misleading when the number of observations is low, as it is for dementia and psychiatric illness euthanasia cases. Fortunately, we have data for more than just the one year.
Since 2012 the Euthanasia Commission has consistently published specific figures for dementia and psychiatric illness cases, so we can compare a rise over four years rather than just one. On this basis as a proportion of total 2012 cases, there has been a 17.9% increase in cancer-related cases, a 1.6% increase in dementia cases, and a 1.0% increase in psychiatric illness cases.
Longitudinal data is even more clear than a single year. It unequivocally refutes Smits' silly claim.
Bull is spread
Does Smits' claim matter much? Won't it just slip into oblivion?
No. Michael Haverluck of the conservative Christian paper OneNewsNow has already picked up Smits' article and repeated her claim as gospel. It remains to be seen how many other anti-euthanasia bloggers republish this nonsense.
Unacceptable conduct
In my view, publishing such a categorical yet false statement — even when unintentional — without first properly checking the facts, is unacceptable conduct. The article (and its derivatives) ought to be withdrawn.
Blog by Neil FrancisPosted on Wednesday 27th April 2016 at 11:36pm
Wesley Smith never seems to tire of spreading opinion. In another piece of published nonsense, he's proposed that USA's rise in national suicide rate is in significant part a consequence of assisted dying law in those few states that permit it (up until the most recent general suicide data that's Oregon, Washington state, Vermont and Montana). His claim flies in the face of actual evidence.
Wesley Smith is a Senior Fellow at the Discovery Institute. Remember that? It's the organisation that a USA Federal court ruled pursues "demonstrably religious, cultural, and legal missions," and which comprehensively lost a test case in which it tried to have 'intelligent design' (that's creationism with lipstick) taught as a 'scientific' alternative to evolution.
In a piece recently published by conservative blog NationalReview and reprinted in pro-life LifeSiteNews, Mr Smith has asserted that assisted suicide has a significant part to play in the rising USA national suicide rate. "Color me decidedly not surprised. We are becoming a pro-suicide culture," he asserts.
"I am convinced that the correlation [between assisted suicide advocacy and the general suicide rate] could also be at least a partial causation."
On the matter of rhetoric, notice how Mr Smith cleverly mixes certainty ('convinced') with uncertainty ('could') in order to hedge his literal argumentative bets while giving the impression of valid authority. Ultimately, however, being certain about uncertainty can only be... uncertain.
Mr Smith argues from a USA Centers for Disease Control (CDC) report that the national suicide rate increased more after 2006, "the very time when the assisted suicide movement has become the most vigorous and made its most dramatic advances [emphasis is Smith's]." He offers not one shred of quantitative empirical evidence to support his contention that the assisted dying movement's 'vigor' changed suddenly and substantially from 2006.
So, what does analysis of relevant and readily-available data show? I've reproduced the USA national general suicide rates obtained from the USA government's CDC online database, plus unemployment rates obtained from the USA government Bureau of Labor Statistics online database in Figure 1. (The suicide data does not include deaths under state Death With Dignity Acts because under these Acts such deaths are not suicides.)
Figure 1: USA national suicide and unemployment rates
The national annual suicide rates are shown in red, and the unemployment rates are shown in blue with linear regression lines for before and after 2006. It's easy to see that prior to 2006 the unemployment rate peaked at around 6%, while after 2006—and clearly in response to the global financial crisis (GFC)—the rate peaks much higher at nearly 10%.
Suicide is indeed a complex phenomenon, with a wide range of both risk factors (e.g. unemployment, mental illness, substance abuse) and protective factors (e.g. mental illness mitigation programs, unemployment benefits), and it would be glib to assert only one or a few factors. Nevertheless, Figure 1 demonstrates a clear correlation between trends in unemployment and the overall suicide rate.
Correlation is of course not causation: though I will in a future report show how extensively common this correlation is around the world and over time. Nevertheless, the data, had Mr Smith bothered looking for it, offers a vastly more rational and compelling explanation of the rise in suicide rate than does some hokey theory about how just 325 rational adults in two states (Oregon and Washington state Death With Dignity Act deaths in 2014) who were already dying and quietly and privately chose to go a little early in response to intolerable suffering, caused the suicide rate amongst 319 million inhabitants (2014) across a nation of fifty states, to rise by a "huge and alarming" amount.
Mr Smith backhandedly acknowledges that there are multiple causes of suicide. "There is no question that assisted suicide advocacy is not the only factor causing this alarming increase in suicides," he says, presumptively positioning his hypothetical reason as definitely one of them.
Mr Smith does refer to a recent journal article by David Jones and David Paton that purports to show a weak link between assisted dying and the total suicide rate (with the weak link appearing only if assisted deaths are counted as suicides). I have analysed that paper in detail and shall deal with it in due course. How it passed peer review (if it was indeed peer reviewed) remains a mystery. The study is of an unacceptably poor standard on a range of facets as I will demonstrate.
In conclusion, did the CDC report that Mr Smith cites suggest that 'assisted suicide contagion' was a possible cause of the increase? Nope.
It's really time that Mr Smith and colleagues gave the misinformation campaign a rest.
Blog by Neil FrancisPosted on Tuesday 19th April 2016 at 2:00am
Lyle Shelton's bunkum tweet is broadcast on ABC's Q&A program
The Managing Director of the Australian Christian Lobby, Mr Lyle Shelton, is at it again.
Yesterday, he tweeted ABC's Q&A program as thousands of people do while it is on air. His tweet was broadcast live to air as shown above. What did he say as panelists were discussing assisted dying law reform?
"Sadly voluntary euthanasia quickly became involuntary euthanasia in Holland. #qanda" LyleShelton
Mr Shelton's claim is bunkum.
Confused language
Firstly, he's confused involuntary with non-voluntary euthanasia.
Involuntary euthanasia is the deliberate hastening of the death of an individual in contravention of the express wishes to the contrary of that individual. Nobody (except the Australian Christian Lobby in its confusion) is seriously suggesting that involuntary euthanasia happens in the Netherlands, even as a 'result' of the country's euthanasia law.
Non-voluntary euthanasia is the deliberate hastening of the death of an individual without an explicit request from that individual. Increased doses of analgesics and sedatives are administered to alleviate intractable symptoms at the end of life, as a result of discussion between doctors and the patient's family (the patient is not currently competent to participate in decisions). The drugs may hasten death and if this happens, life is shortened by hours, or less often, days. Despite claims by some assisted dying opponents that this is unique to the Netherlands, scientific research shows clearly that the practice occurs all over the world and is not 'caused' by voluntary euthanasia laws.
ACL staff sing from the same hymn book
Daniel Flynn, Victorian Director of the Australian Christian Lobby, made a similar claim in a formal submission (#694) to the Victorian Parliament's Inquiry into End Of Life Choices:
"There is sufficient evidence to suggest that involuntary euthanasia is frequent in jurisdictions in which euthanasia has been legalised." [p 4.]
Not a shred—let alone 'sufficient'—evidence was offered to back up this silly myth, though it's hardly surprising given that there isn't any.
What does the evidence actually show?
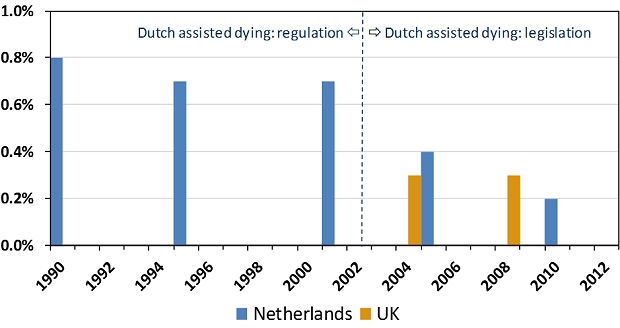
The scientific evidence is crystal clear and it is the opposite of Lyle Shelton and the Australian Christian Lobby's claim. Since around 1985 the Netherlands had permitted assisted dying by regulation: under agreement amongst relevant authorities. The rate of non-voluntary euthanasia remained relatively unchanged under this arrangement (Figure 1). In 2002 the Netherlands' euthanasia Act came into effect, replacing regulatory arrangements with a comprehensive set of legislative (i.e. statutory) requirements.
Figure 1: Netherlands and UK non-voluntary euthanasia rates
Since 2002, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen.1 The drop is statistically significant. The rate of non-voluntary euthanasia in the Netherlands is now around the same level as in the United Kingdom.2 The UK is generally accepted as the world's gold standard in palliative care practice and it does not have an assisted dying law.
Absolutely contrary to the claim of the Australian Christian Lobby's Lyle Shelton, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen. It's now similar to the rate in the UK, which has no assisted dying law.
ABC news standards
Since the ABC moved the Q&A program from its entertainment division to its news division there is a heighted obligation on the broadcaster to ensure that the show's content is reason- and evidence-based, and not merely a platform for anyone to promote silly misinformation in support of a perspective.
No doubt the ABC will rise suitably to the occasion of discouraging misinformation and ensuring that any is corrected.
We'll be watching the next episode of ABC Q&A closely to fact check anything Mr Shelton and others say about assisted dying law reform. Give us a bell if you spot anything you know or suspect is untrue.
---------------
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliative Medicine, vol. 23, no. 3, pp. 198-204.
The F filesPosted on Tuesday 22nd March 2016 at 12:00am
One of the articles wrongly claiming 650 Dutch babies euthanized
Opponents of assisted dying have fallen prey to misinformation contagion about the Dutch Groningen Protocol, claiming that 650 babies would be or are euthanized every year. The claim is comprehensively and evidentially false.
Starting in 2013 and increasing in shrillness in 2015, numerous opponents of assisted dying law reform—many of whom are connected to conservative (Christian) sources—published online articles making false claims about the Dutch Groningen Protocol, wrongly claiming that up to 650 babies could be, would be or actually are ‘euthanized,’ ‘killed’ or ‘murdered’ every year under the Protocol’s provisions.
A national Dutch Regulation (not statute) effective since late 2006 whose current name is so long that it remains convenient to use its old name, ‘Groningen Protocol,’ even though it has changed.
Permits, only as a last resort and with a number of strict conditions, the intentional ending of a newborn’s life when the newborn is in current (not merely anticipated) untreatable and unrelievable extremis.
Mandatory reporting of intentionally hastened deaths to a national Commission and the Board of Prosecutors General at The Hague.
Physician is not cleared until the case is deemed acceptable by the Commission and the Board and the Minister of Security and Justice.
The Regulation is entirely separate from and unrelated to the Dutch Euthanasia Act for competent adults.
Where did the '650 babies euthanized' claim come from?
In 2013 the Royal Dutch Medical Association (KNMG) published a media release that launched a major policy paper about end-of-life decisions for neonates. The media release stated that of the approximately 175,000 births in the Netherlands each year, around 650 newborns will die as a result of severe congenital defects.
Some of these babies die soon after birth, in the delivery room. Others die later in neonatal intensive care despite the best interventions attempting to keep them alive. Yet others die after futile treatment is withdrawn and palliative (comfort) care is administered to minimize suffering prior to death.
Only in a tiny minority of cases is there a medical intervention with an explicit intention to hasten the death of the newborn, who is in untreatable and unrelievable extremis.
Despite this clarity, opponents—mostly linked to conservative religious sources—jumped on the misinformation bandwagon and trumpeted that 650 babies either could be or would be or are actually ‘euthanized,’ ‘killed’ or ‘murdered’ every year in the Netherlands.
What's the actual evidence?
Neonatal euthanasia occurs around the world regardless of prohibition and is not caused by a protocol or regulation
For example, the rate in France, with no regulation, is much higher than the Netherlands.
Intentional hastening of neonatal death in the Netherlands is rare
Most neonatal deaths occur either quickly with no medical intervention, or intensive treatment proves futile and palliative (comfort) care is administered until death.
The (Groningen) Regulation has been further restricted since it was first formulated
It has not been 'relaxed' as claimed by some opponents.
The Regulation is separate from and completely unrelated to the Netherlands' Euthanasia Act
The Euthanasia Act is only for mentally competent adults (and 12-16 year olds with parental agreement).
Physicians do not receive black-letter law protection as they do under the Euthanasia Act
Reporting, investigation and acceptance requirements are even more rigorous than under the Euthanasia Act.
The rate of intention to hasten neonatal death has decreased since the Regulation came into effect
In eight years prior to Regulation there were twenty two reported cases, and only two in eight years since Regulation.
The rate of medical end-of-life decisions with an explicit intention to hasten death was 8–9% prior to Regulation, dropping to 1% after Regulation.
The use of neuromuscular blockers has decreased.
Physicians report improved communication with parents
Shared decision-making and better opportunities for parents to grieve the loss of their child.
There are clear explanations for the decrease in neonatal euthanasia in the Netherlands:
Physicians report they are fearful of prosecution under the Regulation, so they now more often administer palliative care not intended to hasten death.
A folate supplementation program for pregnant females has resulted in a substantial drop in the rate of spina bifida and related disorders.
An antenatal screening program at 20 weeks has resulted in a higher rate of pregnancy terminations for major congenital disorders.
In conclusion
Despite all these facts, in an epidemic of 'confirmation bias' that drove misinformation contagion, many anti-euthanasia commentators have published false claims about '650 babies euthanized' under the Dutch Groningen Protocol. I provide a forensic examination of the issue in the latest edition of the Journal of Assisted Dying.
This is not the first example of how opponents of assisted dying widely circulate information that is untrue (e.g. check out the Council of Europe Declaration 1859 case), and it won't be the last. However, for opponents of assisted dying to avoid egg on face, I'd recommend:
Neonatal deaths under Dutch Groningen Protocol very rare despite misinformation contagion
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 1, no. 1, pp. 7–19.
Abstract
The Groningen Protocol specifies criteria for the potential termination of life in severely ill newborns in extremis with untreatable and unrelievable conditions. In September 2006 the Netherlands formally adopted a Regulation incorporating the Protocol. Despite the Regulation’s development through extensive professional consultation, endorsement by the Dutch Paediatric Association, empirical data showing a decrease rather than increase in use, and research showing that neonatal euthanasia occurs around the world in the absence of regulation, the Dutch Regulation has sparked controversy. More recently it has been claimed that hundreds of babies a year are killed under its provisions. Forensic analysis reveals the claim to be comprehensively and evidentially false. Wide online dissemination of the claim by mostly religious sources demonstrates confirmation bias and misinformation contagion.
Francis, N 2016, 'Neonatal deaths under Dutch Groningen Protocol very rare despite misinformation contagion', Journal of Assisted Dying, vol. 1, no. 1, pp. 7-19.
Blog by Neil FrancisPosted on Saturday 2nd January 2016 at 12:35am
Dr William Toffler (left) acknowledges no slippery slope cause-and-effect evidence, with Drs Bentz and Stevens
A new scholarly journal focused on end-of-life ethics, decision-making and practice has just been launched: the Journal of Assisted Dying. In the first article, claims by Oregon lobby group Physicians for Compassionate Care (PCC), including Doctors Bill (William) Toffler and Ken Stevens (and others) are assessed against empirical evidence and found to be completely wrong, or highly misleading as a result of selective use of data.
The new scholarly journal, the Journal of Assisted Dying, is dedicated to careful and holistic analysis of evidence in regard to the various forms of assisted dying that are lawful in a number of jurisdictions around the world... and to practices in jurisdictions where assisted dying remains illegal.
In the first article of a series on Oregon, I examine claims and speculations made by various doctors (and others who quote them), that Oregon has the second-highest suicide rate in the USA (or is always in the top 10), that Oregon's Death With Dignity Act has resulted a massive increase in the state's general suicide rate, and other astonishing statements.
Of course, the empirical evidence from the Oregon Health Authority and from the USA Centers for Disease Control and Prevention does not support these statements and interpretations, and I analyse and critique the evidence.
Some of the claims are just plain factually and hugely wrong. Others are the result of failing to read their sources more carefully, misunderstanding what the data actually represents. Still further claims are made on the basis of selectively-chosen statements from government reports, while omitting statements that are contrary to, or provide alternative and well-researched explanations for Oregon's recently rising general suicide rate.
Drs Toffler and Stevens have even published some of their claims and speculations in the British Medical Journal.1 It goes to show that even good journals sometimes publish bunkum: their article was a letter to the editor rather than peer-reviewed research. Great care is required to sort real evidence from hype and opinion.
Ultimately, Dr Bill Toffler of PCC has acknowledged on video that there is no cause-and-effect evidence between Oregon's Death With Dignity Act and Oregon's suicide rate, an acknowledgement that went unchallenged by his two PCC colleagues present at the time, Dr Ken Stevens and Dr Chuck (Charles) Bentz. You can see Dr Toffler's statement here (at 10'50").
The Journal of Assisted Dying is an open-access journal, and you can read the full article here.
-----
1. Toffler, WL & Stevens, K 2015, 'Re: Assisted dying: law and practice around the world', BMJ, vol. 351, 19 Aug, p. h4481.
Blog by Neil FrancisPosted on Thursday 17th September 2015 at 6:06am
On 16th September 2015, the Victorian Director of the Australian Christian Lobby (ACL), Dan Flynn, appeared as a witness to the Victorian Parliament’s end of life choices inquiry being conducted by the Legal and Social Issues Committee. He made a number of mistaken statements, but what was most worrisome was the revelation of the ACL’s real agenda: to wind back patient rights more than a quarter century.
In his opening address, Mr Flynn opined that assisted dying was 'not supported' by a 'broad base' of Victorian Christians (not just the ACL). This belief is diametrically at odds with clear and repeated evidence from multiple sources.
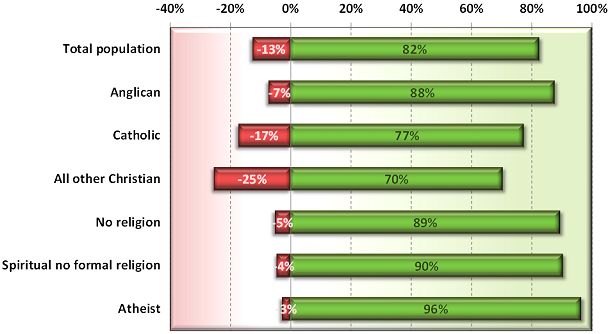
In 2012, I reported on a Newspoll study into Australian attitudes towards assisted dying. Not only did a whopping majority of citizens support assisted dying, but so did a great majority of Anglicans, Catholics and other Christians (Francis 2012).
Newspoll 2012: Australian attitudes to assisted dying law reform by religion (green=support, red=oppose)
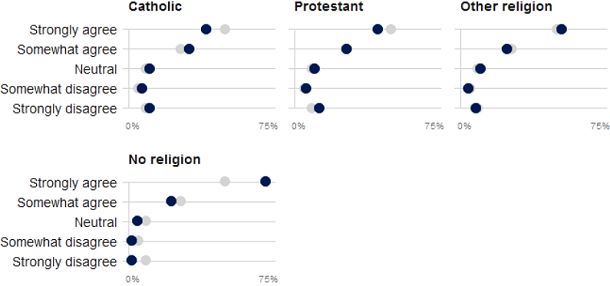
These national results are reflected by a sample of over 60,000 Victorians through the VoteCompass system during the 2014 Victorian election (Stayner 2014). It confirms a substantial majority of Catholics, Protestants, other religious and non-religious Victorians support assisted dying law reform.
VoteCompass 2014: Victorian attitudes to assisted dying law reform by religion (grey=population average)
Out of date
Mr Flynn then referred to a Tasmanian Parliament’s inquiry into assisted dying which rejected law reform. However, the inquiry to which he refers was held in 1998, when Oregon’s Death With Dignity Act had barely been established, the Northern Territory’s Rights of the Terminally Ill Act had been extinguished within just eight months of coming into operation, and the Dutch, Belgian, Luxembourg, Washington and other legislation and judgements did not yet exist.
So, the Tasmanian Parliament’s rejection came from a position of a then general lack of information. The Oregon law has been in effect since 1997, the Netherlands and Belgium since 2002, Washington since 2008, Luxembourg since 2009, and so on. There is now plenty of evidence that assisted dying law reform doesn’t cause slippery slopes that opponents love to theorise about.
Wrong about ‘United Nations’
Mr Flynn then said that the United Nations had in 2012 expressed concern about a ‘lax attitude’ towards euthanasia in Europe, specifically mentioning the Netherlands and Belgium. This is completely untrue. Because it’s easy to make a simple blooper during a presentation, we’ll put aside the fact that he meant to refer to a completely different organisation: the Council of Europe.
We know this because he read directly from Council of Europe declaration 1859 (Council of Europe Parliamentary Assembly 2012). His ACL submission (Australian Christian Lobby 2015) reports (as he read out) exactly one sentence of the declaration, with his added emphasis, as:
"Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited."
But presented in this manner the statement is quite misleading. As I explain in a forensic analysis of the misinformation campaign about this resolution (Francis 2015), the resolution was utterly clear about its intent: it was not about euthanasia (it explicitly said so), but rather about advance care planning. What the resolution spoke against (in the one sentence conveyed above) is non-voluntary euthanasia, not voluntary euthanasia. Both sides of the assisted dying debate agree that non-voluntary euthanasia (one person deciding for a hastened death on behalf of another) is not acceptable. It is not contentious.
In no way did the Council of Europe's resolution critique voluntary euthanasia or comment on any jurisdiction in which it is legal. And, the United Nations source to which the ACL submission refers was released in 2001, fourteen years ago and at the time of the Netherlands' Euthanasia Act was before the Dutch Parliament. With then limited information about how such laws work in practice, it expressed concern about the upcoming Act.
Wrong about Belgium’s law and practice
Mr Flynn referred vaguely to two cases of euthanasia in Belgium in which persons who requested and received euthanasia were not experiencing intolerable pain, which Mr Flynn asserted was a required safeguard in Belgium’s euthanasia Act. This was another supposed example of transgression of safeguards. Wrong again.
While the Belgian Euthanasia Act is officially published only in Dutch and French, a robust English translation has been prepared under the supervision of Professor Herman Nys of the Centre for Biomedical Ethics and Law at the Catholic University of Leuven (see Parliament of Belgium 2002). The word ‘pain’ does not appear in the Act… at all. What does the Act have to say about the legislature’s intent on who may qualify? The relevant clause in Section 1 says:
— "the patient is in a medically futile condition of constant and unbearable physical or mental suffering that can not be alleviated, resulting from a serious and incurable disorder caused by illness or accident."
It’s abundantly clear: mental suffering from an illness or accident qualifies as much as physical suffering, and the suffering does not need to be ‘pain’ as Mr Flynn mistakenly asserted to the Parliamentary Committee.
Mr Flynn also stated that there are mobile end-of-life units in Belgium. There aren’t. (But there are in the Netherlands, and they must follow precisely all the same requirements as anyone else. They operate to provide choice to patients whose regular or reachable doctors disagree with assisted dying and therefore decline to evaluate whether the patient may qualify under the Act.)
Confused about Advance Care Directives
In further testimony, Mr Flynn opined that the degree to which a doctor should be allowed to override a patient’s Advance Care Directive (ACD) is in part influenced by whether the doctor can speak with the patient.
But if the patient can currently speak and participate in decision-making, the advance care directive doesn’t apply: it is mute and of no effect. An ACD only applies when the patient cannot currently participate in their own decision making. That’s (only) what it’s for.
Winding rights back more than a quarter century
But the most worrying aspect Mr Flynn’s testimony was the revelation of ACL’s opposition to the right to refuse unwanted medical treatment.
The Medical Treatment Act 1998 (Vic) has enshrined for now more than twenty five years a patient’s right to refuse any unwanted medical treatments. In 2003 the Supreme Court of Victoria determined that artificial nutrition and hydration (i.e. via tubes) is medical treatment and can therefore be refused under the Act.
But Mr Flynn repeatedly argued that withholding or withdrawing artificial nutrition and hydration, if the patient’s body could ‘absorb’ them, could amount to physician-assisted suicide, and that doctors must be allowed to override refusals. On the matter of patient autonomy, he said that some autonomy rests "with the patients, but a lot of the autonomy in fact is with the doctor”.
When asked if a Jehovah's Witness who refuses a life-saving and simple blood transfusion ought to be allowed to do so, he conceded that they should be entitled to, but that such a case was a “bit of an outlier”. He didn’t explain on what moral grounds one person could refuse a simple procedure to save their life, but another person mustn’t be allowed to even if the likelihood of saving life was doubtful.
So, the ACL’s real agenda is revealed: it recommends winding back the legislative clock more than a quarter century so as to force patients to endure some medical interventions that they don’t want and firmly refuse, if the doctor wishes to proceed.
No wonder the Committee repeatedly questioned Mr Flynn to ensure they had heard and understood his testimony correctly. In conclusion, Committee Chair Edward O’Donohue observed that Mr Flynn’s evidence was “quite surprising” and “quite contrary” to wide evidence already given.
And it’s no wonder that Theo Mackaay, General Secretary of the Victorian Council of Churches—a group of 30 member churches representing mainstream Christianity—criticised the ACL as “fundamentally conservative” and expressed “deep concern that media portrayal of statements from an established and narrow focused lobby group is presented as being representative of the entire Christian community” (Uniting Church in Australia 2011).
-----
References
Australian Christian Lobby 2015, Submission to the Legal and Social Issues Committee on the Inquiry inito End of Life Choices, Parliament of Victoria, Melbourne, pp. 1-17.
Council of Europe Parliamentary Assembly 2012, Resolution 1859 (2012): Protecting human rights and dignity by taking into account previously expressed wishes of patients, Europe, 25 Jan, pp. 2.
Francis, N 2012, Australian public desire for legalisation of assisted dying in restricted circumstances, YourLastRight.com, Melbourne, pp. 11.
Parliament of Belgium 2002, 'The Belgian Act on Euthanasia of May 28th 2002 (unofficial English translation)', Ethical Perspectives, vol. 9, no. 2-3, pp. 182-188.
Uniting Church in Australia 2011, Australian Christian Lobby does not represent all Australian Christians, nor all Christian viewpoints, 8 Dec, Media Room, viewed 11 Dec 2011, <http://blogs.victas.uca.org.au/mediaroom/?p=971>.
Blog by Neil FrancisPosted on Tuesday 8th September 2015 at 5:16am
It was inevitable, the latest attempt by senior British clergy to persuade politicians to reject Lord Joffe’s Assisted Dying for the Terminally Ill Bill. Led by the Archbishop of Canterbury, Justin Welby—whose predecessor Lord Carey now supports the reform—nine clergy sent a letter to ‘remind’ Parliament of supposed terrible consequences.
So what points did the clerics offer to Parliamentarians, and are they valid? Let’s take a look at each of the five ‘reasons’ advanced in order to deny Brits assisted dying choice.
Firstly, the clerics argue that the ‘answer’ is palliative care. Britain boasts the world’s gold standard in palliative care practice and it’s a great credit to practitioners. But the medical literature as well as the experience of the dying and their loved ones is conclusive: palliative care simply can’t always help. Experts say that “relief of suffering remains an elusive goal for many patients” and it’s “clear that improving palliative care will not remove the need for legalizing assisted dying.”
The premise of palliative care is to provide interventions. However, sometimes, not only does interventionism fail to help, it can itself be a source of suffering. And the individual may not want interventions, but rather to alight from the train of terminal illness one or two stops before the inevitable and intolerable terminus.
Secondly, the clerics argue that jurisdictions with assisted dying laws are facing serious problems, including wrongly claiming that the Dutch are now campaigning to include dementia as a basis to seek an assisted death. This right has been enshrined in Dutch law through advance care directives since 2002. In practice, the request is largely declined by doctors.
The clerics complain that dying patients in assisted dying jurisdictions are now using the law—hardly a surprising outcome given the proportion of people now dying of cancer in their later years.
They complain about supposed ‘doctor shopping’ in Oregon. If the patient’s first (or second) doctor declines a request to consider an assisted death on the basis of the doctor’s own convictions, are these clerics suggesting that the patient ought to have their right to lawful assessment denied, because their first doctor or two were religiously opposed?
Thirdly, the clerics argue that the majority of doctors are opposed to assisted dying law reform, ironically pointing out that a quarter to a third of doctors support reform. Why should Brits be denied a choice because two thirds of doctors currently won’t participate in that choice? (What proportion of doctors would participate in abortions, currently legal?) And doctors—who make up fewer than one in two hundred Brits—don’t elect Parliament, so why are their diverse views a case for outright denial?
Let’s name this argument for what it is: an appeal to apparent ‘authority’. Clerical ‘authorities’ (who don’t represent their flocks who are overwhelmingly in favour of reform) are making an appeal of medical ‘authorities’ as the reason to reject something the public believes should be a right. Paternalism indeed.
The fourth argument spreads an icing of hubris on the cake of objections. The clerics argue that the public really don’t understand and don’t know what they mean when the great majority keep saying ‘yes’ to repeated polls on assisted dying law reform.
Public opinion in fact demonstrates the opposite of gullibility: rejection of the attempted scare campaigns of religious ‘authorities’.
Fifthly (and thankfully lastly), the clerics argue that a right to choose assisted dying will inevitably become a duty to choose it. If the theory that ‘a right becomes a duty’ were an argument to reject one right, then all rights would necessarily be rejected on precisely the same principle.
Enshrined in the Mental Capacity Act 2005, Brits already have a right to refuse any medical treatment, even if life-saving. A Jehovah’s Witness may refuse a simple blood transfusion. An elderly person may refuse burdensome surgery. Yet the right to refuse treatment can theoretically become a duty to refuse, in exactly the same manner.
If the clerics genuinely believe their theory then they would argue to Parliament with equal force that the right to refuse medical treatment should be rescinded. Why don’t they?
The real reason for opposing the assisted dying Bill appears in the letter’s preamble: the clerics “hold all human life sacred”, in other words, a ‘gift from God’. Yet contemporary British Social Attitudes surveys reveal that the majority of Brits are not religious.
So the real question for the Parliament is this: should indefensible arguments put forward by a few clerical ‘authorities’ form a basis for denying choice wanted by the overwhelming majority of voters?