Blog by Neil FrancisPosted on Saturday 24th September 2016 at 11:31pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
Against current moves to legalise assisted dying, Australian Catholic Father John George invokes Nazi Germany, resorts to ad hominem attacks to dismiss those who disagree with him, and demands that the Pope’s edicts are binding on everyone regardless of their own faith or world view.
On 24th September 2016, Journalists Greg Brown and Rick Morton published an article in The Australian, Victorian coroner credited with turning tide on euthanasia, summarising recent Australian moves to legalise assisted dying choice.
Catholic Father John George commented on the article online, quoting four sections of the Catholic Church’s catechism that prohibit assisted dying (sections 2276–9).
Pushback
Other readers of The Australian remarked that they respected his view for himself but they had no interest in the Pope’s views given the readers were not Catholic. In fact, repeated polls in Australia have shown that even the great majority of Catholics (three out of four) do not agree with the Vatican on the matter of assisted dying, a matter which Fr George dismisses merely as ‘fickle votes and polls.’
I would remind Fr George that these are not fickle: Australian public opinion in favour of assisted dying choice has been consistently in the majority for now more than four decades.
Fr George further quoted Catholic sources, for example the LJ Goody Bioethics Centre in Perth, Australia, which he failed to mention is, literally, an agency of the Catholic Archdiocese of Perth. He also selectively quoted Palliative Care Australia, failing to mention that they have acknowledged that not all pain and suffering can be eliminated at the end of life, even with the best palliative care.
Ad hominem attack
In response to a rising tide of objections to his musings, including from Mr Ian Wood, a fellow Christian and co-founder of Christians for Voluntary Euthanasia Choice, Fr George resorted to the ad hominem attack: to attack the person (or persons) rather than the arguments. He said:
“The pro euthanasia claque here make professional Nazi propaganda expert Goebbels look like a 5th rate amateur.” — Father John George.
For anyone in the dark, a claque is a group of sycophants hired to applaud a performer or public speaker. How rude. Fr George seems to have neglected to reflect that it is he who is hired to promote the performance of the Vatican. I applaud his right to do so, and I do not compare him to a treacherous propagandist in a murderous wartime regime in order to dismiss his arguments: I address the arguments themselves.
Nazi Germany
Fr George makes repeated mentions of Nazi Germany as a core reason to deny assisted dying choice.
In contrast, several years ago I was chatting at a conference with the pleasant and engaging Peter McArdle, then Research Director of the Australian Catholic Bishop’s Conference. He volunteered that he very much disliked the “Nazi Germany” argument so often used in religious circles, and wished it would stop because in so doing it meant they’d already lost the debate.
I agree. It’s a lazy and indefensible argument: that rational people in a functioning democracy must be denied choice for themselves on the basis of what some murderous regime did against others at the point of a gun.
Indeed, to rely on such a standard would be to equally argue against the right to religious practice, because the Catholic Church, through its inquisition practices (medieval C12th, papal C13th, Spanish C15th, Roman and Portuguese C16th) relied on torture and resulted in confiscation of property and at least tens (if not hundreds) of thousands of executions for witchcraft and heresy.
Ultimate hubris
But the real crux is that Fr George then unequivocally demands that:
“Principles elaborated by the pope are universally applicable.” — Father John George.
This ultimate hubris reveals a profound lack of self-reflection, both personally and organisationally. Even entertaining for a moment the premise that one individual (or even organisation) can tell everyone on the planet how they must live their lives, how would we choose that person or organisation? Why is it less valid for the head of any other branch of Christianity, of Judaism, Islam, Hinduism, Buddhism (or any other religion) or an agnostic (which I am) or an atheist, to set such rules for everyone, overriding other deeply-held beliefs and values?
A keener example of ‘blinded by faith’ would be hard to find.
Conclusion
I argue that Fr John George displays some of the gravest hubris of some members of the Catholic church. I respect and applaud his world views for himself and those who wish to subscribe. But using canonincal arguments (that is, religious arguments demanded as universally true by virtue of the supposed authority that dispensed them) is probably a major contributor to the current flight of people away from organised religion.
More happily, such an attitude is also contributing to accelerating the legalisation of assisted dying choice because folks can see these arguments for what they are. For that I doff my hat to Fr George.
Blog by Neil FrancisPosted on Sunday 28th August 2016 at 12:58am
Brad Mattes' blog containing misleading and evidentially false statements.
The latest misinformation employed by assisted dying opponents is to imply that Belgium’s general suicide rate is high as a consequence of its assisted dying law: i.e. to argue the discredited 'suicide contagion' line which has in the past been peddled about the USA state of Oregon. I have demonstrated that it was false in Oregon, and I equally demonstrate here that it's false in Belgium.
Mr Brad Mattes recently published emotional anti-assisted-dying nonsense in LifeSiteNews. (LifeSiteNews is a Canadian blog site that was established by the conservative Christian Campaign for Life Coalition and which has a primary principle of promoting “traditional Judeo-Christian principles”. Mr Mattes is radio host for Ohio’s Life Issues Institute, an anti-abortion lobby group established by conservative American John C. Willke who claimed that women’s bodies were resistant to pregnancy as a result of rape.)
Putting on the misinformation running shoes
In his blog Mr Mattes quickly establishes a practice of communicating misinformation by first claiming that assisted dying laws have “devastating effects” around the world including Japan and Albania—which don’t have such laws.
He then sprints onwards to the ‘650 babies euthanized in the Netherlands’ claim—which I have already comprehensively exposed as fake in the Journal of Assisted Dying—and then onto the bogus claim that the Netherlands has descended into a mire of ‘killing’ without the patient’s ‘consent,’ contrary to empirical evidence I've published that such actions occur around the world regardless of assisted dying laws, and which have decreased significantly in the Netherlands and Belgium since their assisted dying statutes came into effect in 2002.
Let’s add fries to that
Having served up a lot of fat and salt that might appeal to those on a fast-food anti-assisted-dying diet, he then offers the unqualified statement:
“By the way, Belgium has the second-highest suicide rate (nonrelated to euthanasia) in Western Europe.” — Brad Mattes
The ‘informational’ consequence is unequivocal: by Mr Mattes failing to contextualise this ‘incidental factoid’ in any way, the reader is destined to deduce that it is Belgium’s euthanasia law that causes Belgium’s suicide rate to be the second-highest in Western Europe. In other words, Mr Mattes is another poorly-informed commentator using the 'suicide contagion' line.
But what are the facts?
Depending on the source and year of data, one can certainly argue that Belgium’s general suicide rate is the second-highest in Western Europe. Setting aside for now the serious question of why it is valid to exclude all of the world’s other countries from the comparison, WorldLifeExpectancy.com reports figures that were published in 2014 (Table 1).
Table 1
Country
Suicides*
Finland
15.11
Belgium
14.64
Iceland
14.06
France
12.84
Austria
11.87
Sweden
11.43
Ireland
11.06
Germany
9.59
Switzerland
9.56
Norway
9.28
Denmark
9.19
Luxembourg
9.14
Netherlands
8.54
Portugal
8.49
Turkey
7.92
UK
6.28
Malta
5.75
Spain
5.23
Italy
4.76
Greece
3.86
* Suicides per 100k population, age-adjusted
The table includes all the countries in the wider definition of “Western Europe”, bar four: no suicide statistics are published for Liechtenstein, Monaco, Andorra or San Marino.
As you can see, Belgium is indeed the second-highest. But this begs the question:
If the reason Belgium is the second-highest is due to its assisted dying law, how come Finland, which Mr Mattes doesn't mention by name and which has no such law, is higher?
It also begs the question:
If assisted dying law were the fundamental cause of a high general suicide rate, how come Switzerland (statute since 1942), Luxembourg (statute since 2009) and the Netherlands (practice since the early 1980s and statute since 2002) have rates that are muchlower, all key facts that Mr Mattes also fails to mention?
These are of course indications that the factoid has been included as a cherry-picked morsel of 'proof' because it sounds so compelling as a throw-away sentence amongst the other (false) statements.
But wait, there’s more
We can go further than merely wondering about the country comparisons, by comparing Belgium’s general suicide rate before and after assisted dying law reform. A critical step in establishing causation is to first establish correlation. If there is no correlation, there can be no causation.
Published OECD data shows that in 2013 (the most recent available data), Belgium’s general suicide rate was 16.7 per 100,000 population. What was it before their 2002 law reform? Well in 2000 it was 20.5, in 1990 it was 19.2, … you get the idea.
Has Belgium’s general suicide rate soared (or even increased modestly) since their 2002 assisted dying law came into effect? No. It’s dropped. Indeed, the slight downward trend apparent before the statute came into effect in 2002 has accelerated downward since (Figure 1).
Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Even the headline is misleading
Mr Mattes fails to point out in his blog that assisted dying statutes in Benelux countries (Belgium, the Netherlands and Luxembourg) never restricted access to only the 'terminally ill,' that is, those imminently dying. He also fails to point out that USA states whose laws do restrict assisted dying to the terminally ill—most notably Oregon and Washington—have not changed their statutes in this regard since they came into effect.
Therefore, his headling implying that lawful jurisdictions have broadened their laws from 'only the terminally ill' is also wrong.
Conclusion
Mr Mattes makes multiple false and misleading claims and it’s easy to see his opinion for what it is: an emotional dump that fails to engage with and indeed flies in the face of actual evidence. The latest 'suicide contagion' implication, that assisted dying law causes Belgium’s general suicide rate to be the “second-highest in Western Europe” is evidentially false.
I call on LifeSiteNews to withdraw Mr Mattes' article because it breaches their primary principle:
“1. Accuracy in content is given high priority. News and information tips from readers are encouraged and validated. Valid corrections are always welcome. Writing and research is of a professional calibre.” — LifeSiteNews
Summary of facts
Belgium's general suicide rate is one of the higher ones in Western Europe. However:
At least one country without an assisted dying law has a higher suicide rate, inconsistent with 'suicide contagion' theory.
Other Western Europe countries with assisted dying laws have suicide rates much lower than Belgium's, also at odds with 'suicide contagion' theory.
But the clincher is that the suicide rate in Belgium has dropped, not risen, since their 2002 assisted dying law came into effect.
The F filesPosted on Monday 8th August 2016 at 7:02am
Back in 2013 the High Court of Ireland rejected a legal bid by multiple sclerosis sufferer Marie Fleming to achieve a lawfully-assisted peaceful death.
The Court naturally relied on expert testimony in reaching its judgement, yet its conclusions included a statement containing significant errors of fact.
The erroneous statement
In its judgement,1 the Court made the following statement:
“Above all, the fact that the number of LAWER (“legally assisted deaths without explicit request”) cases remains strikingly high in jurisdictions which have liberalised their law on assisted suicide (Switzerland, Netherlands and Belgium) — ranging from 0.4% to over 1% of all deaths in these jurisdictions according to the latest figures — without any obvious official response speaks for itself as to the risks involved.” [My emphases in bold]
In fact, the Court's judgement is wrong on not one, not two, but three significant matters. But that hasn't stopped opponents of assisted dying law reform from quoting the judgement as though it were factual and persuasive, when it isn't: relying on it because it was made by a High Court—the 'authority bias.'
Consequences
Here are just a few examples of the Court's statement being wielded by assisted dying opponents as though it were conclusive evidence against law reform:
Family First’s submission opposing assisted dying law reform in New Zealand.
Catholic lobbyist Paul Russell and Catholic NSW MP Greg Donnelly in submissions to the Victorian (Australia) Parliament inquiry into end-of-life choices.
Catholic Professor Margaret Somerville in the New England Journal of Medicine,2 repeated by Alex Schadenberg of the Euthanasia Prevention Coalition as well as by Catholic-founded National Right To Life News; and Somerville again in the (Catholic) Newman Rambler.3
These examples illustrate the frequency of quoting the misinformation and how it feeds into and wrongly shapes public policy formation.
Three strikes
So what are the three counts on which the Court's judgement was seriously wrong?
Strike 1: Wrong concept
First, let’s get the concepts right. LAWER is not “legally assisted deaths without explicit request.”
Such nomenclature is an oxymoron. To ‘assist’ is to accommodate, serve or help someone accomplish something. But if there has been no request then one cannot be helping. You can’t ‘assist’ a little old lady across the road if she has expressed no interest in going there: you’d be forcing her across the road. Equally, you can’t ‘assist’ a death if there’s no proper ‘request.’
LAWER in fact stands for “Life-ending Acts Without Explicit Request” (of a competent patient).5 And with the exception of the possible ‘lawfulness’ of the doctrine of double effect, such acts are illegal.
Further, if such acts were legal as the Court’s statement posits, then there would be no need for an “obvious official response” as the Court then concludes. The statement lacks fundamental coherence.
Strike 2: Not ‘strikingly high’
The Court's judgement states unequivocally that LAWER (otherwise known as Non-Voluntary Euthanasia or NVE) rates in Switzerland, the Netherlands and Belgium are ‘strikingly high’, though no comparative yardstick is recorded in the judgement by which one might draw or justify that subjective judgement. Similar 'strikingly high' statements also appear in sections 102 and 104 of the judgement.
There is in fact a scientific study, published in The Lancet in 2003, that provides sound empirical evidence that could have properly informed the Court (Figure 1).6
Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002
As revealed by this study, the NVE rates in Switzerland and the Netherlands were in fact lower than in Denmark, a country which has never had an assisted dying law.
The only country which did appear to have an NVE rate notably higher than the others was Belgium. The research study collected the data for analysis between June 2001 and February 2002. However, Belgium’s Euthanasia Act was not passed by its Parliament until 28th May 2002, well after data collection was complete. Thus, even in describing Belgium’s NVE rate as ‘strikingly high’ compared to a number of other European countries, it cannot be attributed to an assisted dying law because none existed at the time.
In fact, the NVE rate in Belgium had been found to be high back in 1998,7 well before the Bill for the country's Euthanasia Act was even tabled in Parliament.
Further, if assisted dying laws had such effects, it might be expected that the NVE rate would increase the longer that assisted dying laws were in place. In that case the NVE rates in Switzerland (statute since 1942) and the Netherlands (regulation since the early 1980s) would have NVE rates much higher than Belgium’s (statute since 2002). But the exact opposite is true.
Indeed, Rietjens and colleagues8 further concluded in their review of NVE in the Netherlands, Belgium, Denmark and Switzerland that “the use of drugs with the intention to hasten death without an explicit request of the patient is part of medical end-of-life practice in the studied countries, regardless of their legal framework, and it occurs in similar fashion.” The study, published in 2007, would also have been important evidence before the Court.
Strike 3: Not ‘remaining’ high
The Court's judgement states unequivocally that the LAWER (NVE) rate of the three countries ‘remains’ strikingly high. No specific evidence was supplied in the judgement to support this statement. Indeed, the judgement notes:
In section 28 that Dutch NVE had been “consistently declining.”
In section 91 that “the number of LAWER deaths has significantly declined in both [Dutch and Belgian] jurisdictions.”
In section 94 that “the trend in [Dutch] LAWER cases are declining in numbers (from 1,000 in 1990 to 550 in 2005)” and that in Belgium “the number of LAWER cases has declined since legalisation of assisted death.”
In section 101 that the NVE rates of both the Netherlands and Belgium had dropped.
Despite this clear and repeated evidence, the Court summarises in section 96 that the evidence cannot be “regarded as encouraging or satisfactory.”
But what does empirical research tell us about the NVE trends? In both the Netherlands and Belgium, since assisted dying was enshrined in statute and became effective in 2002, the rate of NVE has decreased significantly (Figure 2).7,9-11 In fact, the rate in the Netherlands is now similar to that in the UK, a country which has never had an assisted dying law and which provides the world’s gold standard in palliative care practice.
Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying
These are critical yardsticks by which to judge practice in jurisdictions that have assisted dying laws with jurisdictions that don't. The UK study was published in 2009 and was readily available prior to the High Court’s hearings, yet appears not to have been presented in evidence.
The final (2010) Dutch NVE statistic in Figure 2 may or may not have been available to the Court: it was published in 2012 around the time the Court was taking evidence. The final (2013) Belgian statistic would not have been available to the Court as it was published in 2015.
Conclusion
While the High Court worked diligently within the scope of evidence brought before it:
The Court’s definition of LAWER is incorrect and incoherent;
Its statement that the NVE rates of the Netherlands and Switzerland are ‘strikingly high’ are evidentially wrong when compared with other countries without assisted dying laws;
Its implication that the higher NVE rate in Belgium was caused by assisted dying law reform is evidentially wrong; and
Its statement that the rates remain high is evidentially wrong.
The High Court's judgement does not provide defensible evidence or argument against assisted dying law reform.
Many lobbyists have repeated these incorrect statements, significantly misleading media, policy makers and legislators.
Now that the facts are readily available it’s appropriate to avoid repeating evidentially wrong statements, regardless of the apparent 'authority' of their source.
Summary of facts
LAWER stands for "Life-ending Acts Without Explicit Request". Its practice is similar in countries with and without assisted dying laws.
The NVE rates in the Netherlands and Switzerland are lower than the rate in Denmark, a country which has never had an assisted dying law.
The NVE rate in Belgium appears higher, but was so long before assisted dying law reform and so cannot have been caused by such a law.
The NVE rates of the Netherlands and Belgium have both decreased significantly since their assisted dying statutes came into effect in 2002.
References
High Court of Ireland 2013, Fleming v Ireland & Ors - Determination, [2013] IEHC 2, Dublin.
Boudreau, JD, Somerville, MA & Biller-Andorno, N 2013, 'Physician-assisted suicide: should not be permitted/should be permitted', New England Journal of Medicine, 368(15), pp. 1450-1452.
Somerville, M 2016, 'Killing as kindness: The problem of dealing with suffering and death in a secular society', The Newman Rambler, 12(1), pp. 1-26.
Keown, J 2014, 'A right to voluntary euthanasia? Confusion in Canada in Carter', Notre Dame Journal of Law, Ethics & Public Policy, 28(1), pp. 1-45.
Pijnenborg, L, van der Maas, PJ, van Delden, JJM & Looman, CW 1993, 'Life-terminating acts without explicit request of patient', Lancet, 341(8854), pp. 1196-1199.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, 362(9381), pp. 345-350.
Bilsen, J, Cohen, J, Chambaere, K, Pousset, G, Onwuteaka-Philipsen, BD, Mortier, F & Deliens, L 2009, 'Medical end-of-life practices under the euthanasia law in Belgium', New England Journal of Medicine, 361(11), pp. 1119-1121.
Rietjens, JA, Bilsen, J, Fischer, S, Van Der Heide, A, Van Der Maas, PJ, Miccinessi, G, Norup, M, Onwuteaka-Philipsen, BD, Vrakking, AM & Van Der Wal, G 2007, 'Using drugs to end life without an explicit request of the patient', Death Studies, 31(3), Mar, pp. 205-21.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, 23(3), pp. 198-204.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, 380(9845), pp. 908-915.
Chambaere, K, Vander Stichele, R, Mortier, F, Cohen, J & Deliens, L 2015, 'Recent trends in euthanasia and other end-of-life practices in Belgium', N Engl J Med, 372(12), pp. 1179-1181.
Blog by Neil FrancisPosted on Sunday 8th May 2016 at 9:48pm
Jeanne Smits' completely false statement in LifeSiteNews
Well it didn't take long. Recently I posted a fact-based report card on Dutch euthanasia practice, based on the actual data from the 2015 annual report (and all the earlier reports) of the Dutch Euthanasia Commission. Now, just a few days later, conservative religious opponents have begun publishing completely untrue statements about Dutch euthanasia practice.
Catholic blog LifeSiteNews' 'Paris correspondent' Jeanne Smits has bolted out of the misinformation blocks, assertively and categorically stating in respect of the small increase in number of euthanasia cases from 2014 to 2015, that:
"The rise is mainly due to the increase of euthanasia for demented, elderly people as well as psychiatric patients, two categories that raise even more questions than 'ordinary' euthanasia for untreatable physical pain."
Smits goes on to correctly report that dementia was an underlying factor in 109 of the cases in 2015 (against 81 in 2014) and psychiatric disorders in 56 patients (against 41 in 2014).
The total number of euthanasia cases increased from 5306 in 2014 to 5516 in 2015, an increase of 210 cases. The increase in dementia cases was 28 and in psychiatric disorders was 15. Therefore, underlying dementia accounted for 13% of the increase, and psychiatric disorders 7% of the increase.
Cherry-picking
Smits has cherry-picked just the dementia and psychiatric illness figures and presented them in a way that supports her story arc, painting a bleak picture.
But by no stretch of the imagination does dementia and psychiatric illness account "mainly" for the increase as she categorically states.
What didn't Smits report at all? Cancer: the Netherlands' leading cause of death. In 2015, cancer was the underlying condition in 4000 euthanasia cases, against 3888 in 2014, a rise of 112 cases or 53% of the increase. That compares with dementia at 13% and psychiatric illness at 7% (20% combined), which Smits selectively critiques as a 'sharp rise'.
In no way is Smits' statement true.
No, let's be frank: it's an outright lie. Cancer was the major underlying condition accounting for more than half of the small increase (4%) of cases in 2015.
More evidence refutes the claim
Comparing one years' data with just the preceding years' data can be misleading when the number of observations is low, as it is for dementia and psychiatric illness euthanasia cases. Fortunately, we have data for more than just the one year.
Since 2012 the Euthanasia Commission has consistently published specific figures for dementia and psychiatric illness cases, so we can compare a rise over four years rather than just one. On this basis as a proportion of total 2012 cases, there has been a 17.9% increase in cancer-related cases, a 1.6% increase in dementia cases, and a 1.0% increase in psychiatric illness cases.
Longitudinal data is even more clear than a single year. It unequivocally refutes Smits' silly claim.
Bull is spread
Does Smits' claim matter much? Won't it just slip into oblivion?
No. Michael Haverluck of the conservative Christian paper OneNewsNow has already picked up Smits' article and repeated her claim as gospel. It remains to be seen how many other anti-euthanasia bloggers republish this nonsense.
Unacceptable conduct
In my view, publishing such a categorical yet false statement — even when unintentional — without first properly checking the facts, is unacceptable conduct. The article (and its derivatives) ought to be withdrawn.
Blog by Neil FrancisPosted on Tuesday 19th April 2016 at 2:00am
Lyle Shelton's bunkum tweet is broadcast on ABC's Q&A program
The Managing Director of the Australian Christian Lobby, Mr Lyle Shelton, is at it again.
Yesterday, he tweeted ABC's Q&A program as thousands of people do while it is on air. His tweet was broadcast live to air as shown above. What did he say as panelists were discussing assisted dying law reform?
"Sadly voluntary euthanasia quickly became involuntary euthanasia in Holland. #qanda" LyleShelton
Mr Shelton's claim is bunkum.
Confused language
Firstly, he's confused involuntary with non-voluntary euthanasia.
Involuntary euthanasia is the deliberate hastening of the death of an individual in contravention of the express wishes to the contrary of that individual. Nobody (except the Australian Christian Lobby in its confusion) is seriously suggesting that involuntary euthanasia happens in the Netherlands, even as a 'result' of the country's euthanasia law.
Non-voluntary euthanasia is the deliberate hastening of the death of an individual without an explicit request from that individual. Increased doses of analgesics and sedatives are administered to alleviate intractable symptoms at the end of life, as a result of discussion between doctors and the patient's family (the patient is not currently competent to participate in decisions). The drugs may hasten death and if this happens, life is shortened by hours, or less often, days. Despite claims by some assisted dying opponents that this is unique to the Netherlands, scientific research shows clearly that the practice occurs all over the world and is not 'caused' by voluntary euthanasia laws.
ACL staff sing from the same hymn book
Daniel Flynn, Victorian Director of the Australian Christian Lobby, made a similar claim in a formal submission (#694) to the Victorian Parliament's Inquiry into End Of Life Choices:
"There is sufficient evidence to suggest that involuntary euthanasia is frequent in jurisdictions in which euthanasia has been legalised." [p 4.]
Not a shred—let alone 'sufficient'—evidence was offered to back up this silly myth, though it's hardly surprising given that there isn't any.
What does the evidence actually show?
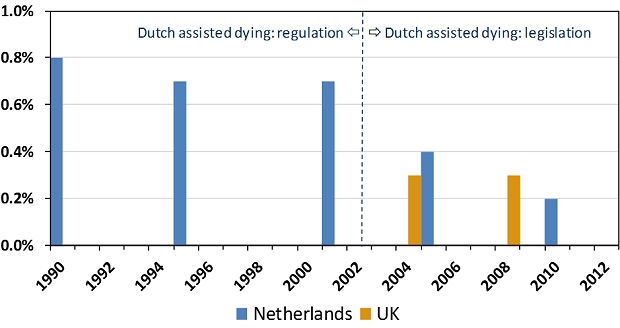
The scientific evidence is crystal clear and it is the opposite of Lyle Shelton and the Australian Christian Lobby's claim. Since around 1985 the Netherlands had permitted assisted dying by regulation: under agreement amongst relevant authorities. The rate of non-voluntary euthanasia remained relatively unchanged under this arrangement (Figure 1). In 2002 the Netherlands' euthanasia Act came into effect, replacing regulatory arrangements with a comprehensive set of legislative (i.e. statutory) requirements.
Figure 1: Netherlands and UK non-voluntary euthanasia rates
Since 2002, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen.1 The drop is statistically significant. The rate of non-voluntary euthanasia in the Netherlands is now around the same level as in the United Kingdom.2 The UK is generally accepted as the world's gold standard in palliative care practice and it does not have an assisted dying law.
Absolutely contrary to the claim of the Australian Christian Lobby's Lyle Shelton, the rate of non-voluntary euthanasia in the Netherlands has dropped, not risen. It's now similar to the rate in the UK, which has no assisted dying law.
ABC news standards
Since the ABC moved the Q&A program from its entertainment division to its news division there is a heighted obligation on the broadcaster to ensure that the show's content is reason- and evidence-based, and not merely a platform for anyone to promote silly misinformation in support of a perspective.
No doubt the ABC will rise suitably to the occasion of discouraging misinformation and ensuring that any is corrected.
We'll be watching the next episode of ABC Q&A closely to fact check anything Mr Shelton and others say about assisted dying law reform. Give us a bell if you spot anything you know or suspect is untrue.
---------------
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, vol. 380, no. 9845, pp. 908-915.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliative Medicine, vol. 23, no. 3, pp. 198-204.
The F filesPosted on Tuesday 22nd March 2016 at 12:00am
One of the articles wrongly claiming 650 Dutch babies euthanized
Opponents of assisted dying have fallen prey to misinformation contagion about the Dutch Groningen Protocol, claiming that 650 babies would be or are euthanized every year. The claim is comprehensively and evidentially false.
Starting in 2013 and increasing in shrillness in 2015, numerous opponents of assisted dying law reform—many of whom are connected to conservative (Christian) sources—published online articles making false claims about the Dutch Groningen Protocol, wrongly claiming that up to 650 babies could be, would be or actually are ‘euthanized,’ ‘killed’ or ‘murdered’ every year under the Protocol’s provisions.
A national Dutch Regulation (not statute) effective since late 2006 whose current name is so long that it remains convenient to use its old name, ‘Groningen Protocol,’ even though it has changed.
Permits, only as a last resort and with a number of strict conditions, the intentional ending of a newborn’s life when the newborn is in current (not merely anticipated) untreatable and unrelievable extremis.
Mandatory reporting of intentionally hastened deaths to a national Commission and the Board of Prosecutors General at The Hague.
Physician is not cleared until the case is deemed acceptable by the Commission and the Board and the Minister of Security and Justice.
The Regulation is entirely separate from and unrelated to the Dutch Euthanasia Act for competent adults.
Where did the '650 babies euthanized' claim come from?
In 2013 the Royal Dutch Medical Association (KNMG) published a media release that launched a major policy paper about end-of-life decisions for neonates. The media release stated that of the approximately 175,000 births in the Netherlands each year, around 650 newborns will die as a result of severe congenital defects.
Some of these babies die soon after birth, in the delivery room. Others die later in neonatal intensive care despite the best interventions attempting to keep them alive. Yet others die after futile treatment is withdrawn and palliative (comfort) care is administered to minimize suffering prior to death.
Only in a tiny minority of cases is there a medical intervention with an explicit intention to hasten the death of the newborn, who is in untreatable and unrelievable extremis.
Despite this clarity, opponents—mostly linked to conservative religious sources—jumped on the misinformation bandwagon and trumpeted that 650 babies either could be or would be or are actually ‘euthanized,’ ‘killed’ or ‘murdered’ every year in the Netherlands.
What's the actual evidence?
Neonatal euthanasia occurs around the world regardless of prohibition and is not caused by a protocol or regulation
For example, the rate in France, with no regulation, is much higher than the Netherlands.
Intentional hastening of neonatal death in the Netherlands is rare
Most neonatal deaths occur either quickly with no medical intervention, or intensive treatment proves futile and palliative (comfort) care is administered until death.
The (Groningen) Regulation has been further restricted since it was first formulated
It has not been 'relaxed' as claimed by some opponents.
The Regulation is separate from and completely unrelated to the Netherlands' Euthanasia Act
The Euthanasia Act is only for mentally competent adults (and 12-16 year olds with parental agreement).
Physicians do not receive black-letter law protection as they do under the Euthanasia Act
Reporting, investigation and acceptance requirements are even more rigorous than under the Euthanasia Act.
The rate of intention to hasten neonatal death has decreased since the Regulation came into effect
In eight years prior to Regulation there were twenty two reported cases, and only two in eight years since Regulation.
The rate of medical end-of-life decisions with an explicit intention to hasten death was 8–9% prior to Regulation, dropping to 1% after Regulation.
The use of neuromuscular blockers has decreased.
Physicians report improved communication with parents
Shared decision-making and better opportunities for parents to grieve the loss of their child.
There are clear explanations for the decrease in neonatal euthanasia in the Netherlands:
Physicians report they are fearful of prosecution under the Regulation, so they now more often administer palliative care not intended to hasten death.
A folate supplementation program for pregnant females has resulted in a substantial drop in the rate of spina bifida and related disorders.
An antenatal screening program at 20 weeks has resulted in a higher rate of pregnancy terminations for major congenital disorders.
In conclusion
Despite all these facts, in an epidemic of 'confirmation bias' that drove misinformation contagion, many anti-euthanasia commentators have published false claims about '650 babies euthanized' under the Dutch Groningen Protocol. I provide a forensic examination of the issue in the latest edition of the Journal of Assisted Dying.
This is not the first example of how opponents of assisted dying widely circulate information that is untrue (e.g. check out the Council of Europe Declaration 1859 case), and it won't be the last. However, for opponents of assisted dying to avoid egg on face, I'd recommend:
Neonatal deaths under Dutch Groningen Protocol very rare despite misinformation contagion
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 1, no. 1, pp. 7–19.
Abstract
The Groningen Protocol specifies criteria for the potential termination of life in severely ill newborns in extremis with untreatable and unrelievable conditions. In September 2006 the Netherlands formally adopted a Regulation incorporating the Protocol. Despite the Regulation’s development through extensive professional consultation, endorsement by the Dutch Paediatric Association, empirical data showing a decrease rather than increase in use, and research showing that neonatal euthanasia occurs around the world in the absence of regulation, the Dutch Regulation has sparked controversy. More recently it has been claimed that hundreds of babies a year are killed under its provisions. Forensic analysis reveals the claim to be comprehensively and evidentially false. Wide online dissemination of the claim by mostly religious sources demonstrates confirmation bias and misinformation contagion.
Francis, N 2016, 'Neonatal deaths under Dutch Groningen Protocol very rare despite misinformation contagion', Journal of Assisted Dying, vol. 1, no. 1, pp. 7-19.
The F filesPosted on Friday 11th March 2016 at 9:42pm
He was red in the face and the veins on his neck were standing out. He involuntarily spat as he shouted while furiously jabbing a scientific journal paper high into the air. “This paper proves that palliative sedation doesn’t hasten death!,” he bellowed from the audience.
The recipient of the Catholic priest’s[§] ire was Dr Rodney Syme, who had just delivered a paper at a Catholic bioethics conference in Melbourne, Australia.
The presentation didn't win over an already skeptical audience given that his address was to argue, by referring to the scientific literature, that palliative care can’t always help alleviate refractory end-of-life symptoms and that continuous deep sedation (CDS) may hasten a patient’s death.
By the end of the address the audience was bristling with hostility and our priest bolted to his feet to commence the attack.
I hadn’t seen the journal paper the priest was brandishing, so immediately after the conference I retrieved a copy and studied it.1 You can obtain your own copy here.
But first, a little background on the doctrine of double effect.
Doctrine of double effect
There has been ongoing debate—both scholarly and otherwise—about whether CDS (particularly the administration of higher doses of opioids) for dying patients may hasten their death. CDS may be administered where the dying patient is suffering from intolerable and otherwise unrelievable symptoms, for the purpose of relief from those symptoms through the cessation of consciousness, even if it might hasten the patient's death.
To some, this is an uncontroversial medical intervention supported by the doctrine of double effect. The doctrine is widely attributed to thirteenth century Catholic Saint Thomas Aquinas, though he probably developed it from ancient Roman principles.
The doctrine says that it is acceptable to take this kind of action if it is proportionate to the suffering of the patient, that there are no other
less problematic alternatives, and that the doctor's intention is to relieve the suffering and not to hasten the patient’s death.
Skeptics of the doctrine point out that it can’t be reliably determined what the doctor was actually intending when they administered CDS prior to death. They also identify that the notion that it’s OK for a doctor to kill their patient (hasten her death) as long as the doctor “doesn’t really mean to,” is ethically questionable.
So, on the one hand the doctrine of double effect is relied upon to defend doctor actions, and on the other, it is claimed that CDS doesn’t hasten death in any case.
That’s having your cake and eating it too. If CDS didn’t hasten death, doctors wouldn’t need the doctrine of double effect as a defense.
Poor methodology
Back to the brandished paper. Having read it, I don’t understand how this paper passed peer review, assuming it was indeed peer reviewed. It’s a fact of life that on occasion, even prestigious journals like Lancet and the Journal of the American Medical Association publish manuscripts that shouldn’t see the light of day. I argue that this article (from Annals of Oncology) is one of them.
The research suffers from multiple, serious methodological problems.
The research suffers from multiple, serious methodological problems. Sure, the researchers attempted to match test patients (who received CDS) with control patients (who didn’t receive CDS), by age, class, gender, reason for admission and for functional status. But there the good work ends.
Here are some of the serious methodological flaws in the study.
Primary measure invalid. The authors report that they measured patient survival time from admission to hospice until death from any cause. This alone invalidates the entire study. If you say you are measuring the effects of CDS, then you have to measure from the commencement of CDS, not from some other event that is not the substance of your test.
Insufficient inclusion control. There is so much variability amongst the test and control subjects that the possibility of sufficient sensitivity to detect differences is highly unlikely. For example, around half of patients (53%) were admitted for uncontrolled symptoms of many and varied kinds but were not imminently dying, while a large minority (41%) were imminently dying. There was a wide range of cancer types from slow to aggressive, and of metastatic sites. The sheer breadth of patient contexts gave rise to a survival standard deviation (68% of observed variance, 6 days) that was 50% larger than the mean survival period (4 days). Translating that into 95% confidence (two standard deviations), the variance was three times larger (12 days) than the mean (4 days). Put another way, at 95% confidence, patients survived from minus 8 days to plus 16 days (from admission, not administration of CDS). Hardly the stuff to drive assertive conclusions.
Insufficient intervention assessment. The researchers considered only the administration of sedatives, not of any other medical or palliative interventions in their assessment of patient survival. What other interventions were administered, when and in what amount, and how successful were they? The authors also assumed that any necessary nutrition and hydration was given to patients (whether natural or by tube) equally across hospice units because “the best palliative care should be provided.” There was no mention of whether the various units had identical (or any) written palliative care practice standards or whether those standards were known and actually practiced by attending physicians and nurses in patient cases for this study.
Insufficient intervention control. A wide range of sedative types (not just opioids) were administered in a wide range of doses for widely ranging periods of time; from sudden, light and intermittent, to heavy and continuous. Around half the patients receiving sedation received multiple different sedatives.
It is hardly surprising then, given this sorry state of affairs, that the study failed to find a significant difference in ‘survival’ between test and control groups: the design was certain to result in insufficient sensitivity. (Curiously, the CDS patients survived on average longer (12 days) than the control patients (9 days), though the difference was not statistically significant.)
Unscientific conclusion
In scientific studies—particularly those which have yet to be successfully replicated by other researchers—best practice dictates that the minimum ‘significance’ is cautiously attributed to the results. The minimum significance in this case would be that “our study did not find evidence to support the contention that administration of sedation hastens patient death”.
The conclusion asserted by the researchers
is not established by the study.
The next level of attribution is still cautious, but a little more assertive: “the results suggest that the administration of sedation doesn’t hasten patient death”. It is my belief, especially given the poor design and conduct of the study, that this level of attribution would be too high.
But the authors went all out. They categorically concluded that “PST [palliative sedation therapy] does not shorten life” and trumpeted it in the article’s title: “Palliative sedation therapy does not hasten death.” On the basis of this unjustifiable interpretation they further categorically concluded that the doctrine of double effect is therefore unnecessary.
The authors in my view committed a serious scientific blunder in translating an exploratory and poorly-designed study into unqualified and assertive, unsupported conclusions. How this passed peer and editorial review is a mystery.
The upshot
The upshot of this is that our priest, perhaps with an understandable deficit of expertise in scientific endeavour, grabbed a paper that supported his hypothesis and fervently believed it to provide unarguable evidence, given its unequivocal title and conclusion.
In reality, each and every paper published in scientific journals has to be read and judged on its own merits. It is not appropriate to simply accept a study’s conclusions merely by virtue of its publication in a journal, even a prestigious one.
In reality, each and every paper published in scientific journals has to be read and
judged on its own merits.
Critical appraisal (including cross-checking other sources) is the scientific standard of practice I employ as I follow trains of research and commentary on various facets of end-of-life decisions and assisted dying, across my literature collection now well in excess of five thousand journal articles, theses, books, professional policy papers and other sources.
It is a standard I commend to everyone in order to hone in on the truth and to avoid dissemination of flapdoodle, fudge and fiction.
References
1 Maltoni, M, Pittureri, C, Scarpi, E, Piccinini, L, Martini, F, Turci, P, Montanari, L, Nanni, O & Amadori, D 2009, 'Palliative sedation therapy does not hasten death: results from a prospective multicenter study', Ann Oncol, 20(7), pp. 1163-9.
[§] The meeting was conducted under Chatham House rules, so what was said can be reported, but who said it cannot.
Blog by Neil FrancisPosted on Saturday 2nd January 2016 at 12:35am
Dr William Toffler (left) acknowledges no slippery slope cause-and-effect evidence, with Drs Bentz and Stevens
A new scholarly journal focused on end-of-life ethics, decision-making and practice has just been launched: the Journal of Assisted Dying. In the first article, claims by Oregon lobby group Physicians for Compassionate Care (PCC), including Doctors Bill (William) Toffler and Ken Stevens (and others) are assessed against empirical evidence and found to be completely wrong, or highly misleading as a result of selective use of data.
The new scholarly journal, the Journal of Assisted Dying, is dedicated to careful and holistic analysis of evidence in regard to the various forms of assisted dying that are lawful in a number of jurisdictions around the world... and to practices in jurisdictions where assisted dying remains illegal.
In the first article of a series on Oregon, I examine claims and speculations made by various doctors (and others who quote them), that Oregon has the second-highest suicide rate in the USA (or is always in the top 10), that Oregon's Death With Dignity Act has resulted a massive increase in the state's general suicide rate, and other astonishing statements.
Of course, the empirical evidence from the Oregon Health Authority and from the USA Centers for Disease Control and Prevention does not support these statements and interpretations, and I analyse and critique the evidence.
Some of the claims are just plain factually and hugely wrong. Others are the result of failing to read their sources more carefully, misunderstanding what the data actually represents. Still further claims are made on the basis of selectively-chosen statements from government reports, while omitting statements that are contrary to, or provide alternative and well-researched explanations for Oregon's recently rising general suicide rate.
Drs Toffler and Stevens have even published some of their claims and speculations in the British Medical Journal.1 It goes to show that even good journals sometimes publish bunkum: their article was a letter to the editor rather than peer-reviewed research. Great care is required to sort real evidence from hype and opinion.
Ultimately, Dr Bill Toffler of PCC has acknowledged on video that there is no cause-and-effect evidence between Oregon's Death With Dignity Act and Oregon's suicide rate, an acknowledgement that went unchallenged by his two PCC colleagues present at the time, Dr Ken Stevens and Dr Chuck (Charles) Bentz. You can see Dr Toffler's statement here (at 10'50").
The Journal of Assisted Dying is an open-access journal, and you can read the full article here.
-----
1. Toffler, WL & Stevens, K 2015, 'Re: Assisted dying: law and practice around the world', BMJ, vol. 351, 19 Aug, p. h4481.
Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 1, no. 1, pp. 1–6.
Abstract
Background: Several physicians have speculated that Oregon’s general suicide rate is evidence of suicide contagion as a result of Oregon’s Death With Dignity Act (‘the Act’). Methods: Search and analysis of physician and related online sources of Oregon suicide contagion speculation; retrieval and analysis of cited Centers for Disease Control and Prevention (CDC) and other publications relied upon; analysis of authoritative, public Government mortality data for Oregon and other USA states. Results: Several physicians have speculated about Oregon suicide statistics in a manner that is not supported by the cited publications, or by public CDC mortality database data. The claims variously (a) misrepresent key data in the publications, (b) omit information in the publications that is at variance with suicide contagion speculation, and (c) overlook other significant information at variance with speculation. The physicians have previously acknowledged inability to prove perceived “slippery slope” effects of the Act. Other opponents of the Act have republished the physicians’ erroneous information. Conclusions: Evidence advanced by several physicians to speculate that Oregon’s Death With Dignity Act causes suicide contagion in Oregon is variously false, misleading or highly selective—omitting key facts—and has arisen even though the physicians acknowledge they have no proof of ‘slippery slope’ effects.
Article keywords
suicide contagion, copycat suicide, Werther effect, slippery slope, misinformation, Oregon, Dr William Toffler, Dr Kenneth Stevens, Physicians for Compassionate Care
Full PDF
Download the full PDF: (390Kb)
Citation
Francis, N 2016, 'Physician use of misinformation to speculate 'assisted dying suicide contagion' in Oregon', Journal of Assisted Dying, vol. 1, no. 1, pp. 1-6.
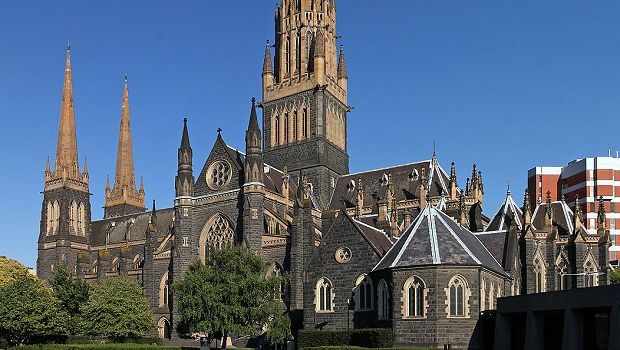
 Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Figure 1: The Belgium general suicide rate before and after assisted dying law reform Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002
Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002 Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying
Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying