Netherlands 'suicide contagion' from assisted dying: Theo Boer's smoke and mirrors
Author(s)
Neil Francis
Journal
Journal of Assisted Dying, vol. 4, no. 1, pp. 1–11.
Abstract
Background: Concerns had been raised about the scientific quality of a 2017 article by ethicist Theo Boer in which he theorised that lawful voluntary assisted dying (VAD) would potentially ‘dampen’ suicide rates, but drew the opposite conclusion: the suggestion that VAD cases have caused higher suicide rates. Methods: A structured, forensic examination of the article was conducted. Results: Numerous serious shortcomings were found, including (a) profound unfamiliarity with the complexity of suicide; (b) lack of a clear and specific pre-hoc methodology; (c) numerous unsupported speculations; (d) cherry-picked data and casual dismissal of data at odds with the conclusion; (e) a simple correlation interpreted as causation while failing to control for any confounding factors; (f) incoherent, contradictory and misleading statements; and (g) multiple editorial errors. Conclusions: Boer’s article is poorly conceived and carelessly assembled, revealing unfamiliarity with both the subject matter and with scientific principles. The conclusions drawn are not supported by the article’s methodology or data. The article offers mere smoke and mirrors to conclude that VAD may increase suicide rates, at odds with wider evidence.
Francis, N 2019, 'Netherlands "suicide contagion" from assisted dying: Theo Boer's smoke and mirrors', Journal of Assisted Dying, vol. 4, no. 1, pp. 1-11.
Blog by Neil FrancisPosted on Tuesday 19th September 2017 at 10:30pm
The Age reports on the three AMA dcotors' appearance at Spring Street
As reported in The Age, on Tuesday this week three AMA doctors fronted the Victorian Parliament to spread the word about their perceived horrors of an assisted dying law. Their arguments don’t hold water and politicians should see them for what they are: utter nonsense.
Doctors Stephen Parnis, Mukesh Haikerwal and Mark Yates say they will continue to lobby politicians.
With what?
Here is the ‘substance’ of their arguments — a sticky blomonge of the same old confected and discredited claims.
The vulnerable will be at risk
Dr Parnis said that such a law “puts the most frail and vulnerable in our community — the dying — at profound risk,” pointing to coercion, and patients not getting the medical care they need.
As I’ve explained before, the claim is flapdoodle — circular nonsense.
It’s a circular argument (a logical fallacy) because “the vulnerable” are by definition those “at risk” and vice versa. While the circularity makes the claim about assisted dying risks seem true, it's a false imputation.
By way of comparison, we could equally say that “the vulnerable will be at risk if we wear yellow socks on Wednesdays,” so we should outlaw that as well. Or anything else of which we disapprove and make our argument seem valid by attaching it to “the vulnerable being at risk.”
Let’s not talk about it
Dr Yates argued that the Parliament should not be pursing “divisive legislation.” That’s also a false argument because it's merely an appeal to emotion: avoiding legislating anything upon which there is any disagreement and discomfort. The consequence of this argument is to not legislate at all.
Patient trust in doctors
They also argued that assisted dying legislation would “change the doctor-patient relationship” — by which they mean “damage the relationship,” or they wouldn’t have mentioned it.
Again, as I have shown before, the empirical evidence from around the world is consistent with improved, not damaged, patient trust in doctors where assisted dying is legal.
The massive AMA flip-flop
But, as I’ve also pointed out before, the real telltale of the AMA doctors’ farcical representation to the Victorian Parliament is this: while opposing assisted dying legislation because patients might be pressured, subtly or otherwise, to choose death, the AMA officially endorses the right to refuse medical treatment, which includes life-saving treatment.
The hypothetical risk of patients being encouraged to refuse life-saving medical treatment is identical in kind to that of assisted dying. Yet in Victoria, the right to refuse is protected by just three statutory safeguards, while the assisted dying legislation is founded on no fewer than 68 safeguards.
So the AMA incoherently promotes one hypothetical pressure-to-die pathway with only three protections, while cruelly opposing a parallel path with an armada of protections. Let's award 10 out of 10 for the impressive flip-flop manoeuvre.
Conclusion
The AMA doctors’ claims are without merit and advancing them does no favours to their professional credibility.
The F filesPosted on Monday 27th March 2017 at 8:50pm
Dr Michael Gannon announces the AMA's policy review to AMA members in 2015
In 2016, the Australian Medical Association (AMA) reviewed its policy on ‘euthanasia and physician assisted suicide.’ Despite ample evidence to the contrary, the AMA executive set its policy as opposed to assisted dying, when the only position that would have acknowledged and respected the views of most of its membership was a position of neutrality.
The Australian Medical Association (AMA) has been historically opposed to legislative reform that would permit doctor-assisted dying for patients in unremitting and untreatable extremis. Its hostile position had been expressed through a Position Statement (PS) in effect for at least a decade, although its Code of Ethics has been completely silent on the matter.
The AMA’s opposition to doctor-assisted dying has been one of the factors leading to the failure of a number of attempts at assisted dying law reform.
In 2015 the AMA announced a review of its ‘policy’ on ‘euthanasia and doctor assisted suicide,’ managed through its Federal Council. The review was conducted from late 2015 and throughout 2016. It included an online survey of more than 3,700 Australian doctors.
Deeply flawed survey — against assisted dying
The survey methodology contained, however unconsciously, multiple serious design flaws biased against assisted dying: flaws which were brought to the attention of the AMA executive separately by two survey design experts. The executive dismissed the criticisms, incoherently arguing that while the AMA’s reviews are “fully-informed decisions based on well-researched, comprehensive information,” the survey was “not formal ‘research’ as such” and merely a “means to engage our members.”
The AMA relied on selected statistics from the survey to publicly explain the outcome of its review. It also provided its own members a private, detailed report of the review, of which more than half was a comprehensive statistical analysis of the survey.
The ‘Survey Limitations’ section of the report mentioned several minor issues, but not the significant biases brought to the attention of the executive by experts.
Yet supportive doctor responses
Despite these significant biases against assisted dying, the survey found:
68% of doctors said that even with optimal care, complete relief of suffering is not always possible.
60% of doctors said that if lawful, euthanasia should be provided by doctors, and more than half of them (total 32%) said that they would indeed practice it.
52% of doctors said that euthanasia can form a legitimate part of medical care.
50% of doctors expressly disagreed with the AMA’s statement that “doctors should not provide euthanasia under any circumstances.”
38% of doctors expressly disagreed with the AMA’s policy opposed to assisted dying (only half expressly agreed), and 35% of doctors said that euthanasia should be lawful.
Some doctors oppose legalisation, not euthanasia itself
In relation to the last point, other scholarly research has found that an additional 25% of Australian doctors are opposed to law reform not because they are opposed to assisted dying itself, but because they would rather practice it in private without regulatory ‘interference.’ This confirms that more than half of Australian doctors believe assisted dying can be a legitimate and practical part of medical care.
AMA not representative of Australian doctors
Only AMA members were invited and permitted to participate in the survey, and more than 70% of Australian doctors are not AMA members, despite the AMA expressly advancing itself as representing all Australian doctors. Non-members are likely to be more supportive of assisted dying — snubbing AMA membership due to the AMA’s ‘officially’ hostile stance.
Hostile tweets by President during review
During the review process, AMA President Dr Michael Gannon made repeated public statements hostile towards assisted dying, including a statement that doctor assisted dying would offend the Declaration of Geneva. The Declaration has nothing specific to say about assisted dying, and any general Declaration statements Dr Gannon relied upon would be equal arguments against abortion. Yet the AMA accepts abortion practice by doctors.
Indefensible conclusion by AMA Executive
Finally, in the face of ample evidence (despite the methodological biases) that at least half of the AMA’s own members favour doctor involvement in lawful assisted dying and deem it legitimate medical care, and 38% of its own members expressly disagreeing with its opposed policy, the AMA executive decided to maintain ‘official’ organisational opposition in the revised PS.
The PS, which was previously named broadly as about ‘end of life care’, is now exclusively named as about ‘euthanasia and physician assisted suicide,’ even though it continues its broad coverage. This suggests that, however unconsciously, the executive’s attitudes against assisted dying have become more entrenched.
The PS continues to unequivocally state as before that “The AMA believes that doctors should not be involved in interventions that have as their primary intention the ending of a person’s life.” In announcing the conclusions of its review the AMA has promoted this statement widely and as though it applies to all Australian doctors, most of whom are not AMA members.
Neither AMA 'policy' nor its Code of Ethics is binding
Despite the confidence and certainty of the statement, the AMA advises that neither Australian doctors in general nor even its own members are bound by its PSs. Thus, statements in AMA PSs are more ‘suggestions’ or ‘thought bubbles’ rather than authoritative statements.
More recently, the AMA’s Code of Ethics has been updated, yet remains entirely silent on doctor-assisted dying, in curious contradiction of the ‘certainty’ of its PS. The Code of Ethics is not binding on doctors (even AMA members), either.
Incoherent demands for policy consultation
The AMA executive continues to demand deep involvement in the development of a legal framework for assisted dying (despite saying that doctors should not be involved in the practice), yet it has developed no specific frameworks for three other related, already-lawful medical practices: refusal of life-preserving medical treatment, continuous deep sedation until death, and the voluntary refusal of food and fluids.
These discrepancies collectively raise the question as to whether the AMA’s ‘official’ opposition to assisted dying law reform is political rather than medical.
Conclusison
The evidence is clear that the only “justifiable” position the AMA executive could have taken was to declare the AMA neutral towards lawful assisted dying — a matter of individual conscience for its member doctors.
Australian doctors may well question the AMA executive as to how such a flawed process arrived at the outcome it did, and a collection of questions are posed for the AMA to answer. Sixteen questions are posed below.
Why does the AMA, through its Tasmanian representative, think it appropriate to state on national television that dying patients in extremis and without relief can suicide by themselves, even if the AMA doesn’t “encourage” it?
Why did the AMA repeatedly delete corrections to its negative MJA misinformation about assisted dying practice in Belgium?
Why did the AMA decide to review its “policy on euthanasia and physician assisted suicide” when it didn’t specifically have one? It had a policy on the role of doctors in end of life care.
Why did the AMA review comprehensively ignore the substantial secondary data that already exists about the attitudes and practices of doctors and patients in end of life decisions?
Why did the AMA not proactively obtain professional advice and assistance with the design and conduct of its doctor survey, and prefer to use such an amateurish one?
If the AMA really represents all Australian doctors, why did it expressly exclude more than two thirds of them from its survey?
Why did the AMA persistently use inappropriate language and inadequate definitions about assisted dying?
Why did the AMA not make any serious attempt to understand patient perspectives beyond superficial statements that ‘opinions are divided’?
Why did the AMA not report the multiple significant biases in its survey, which it knew about, in the ‘limitations’ section of its final report?
Why did the AMA President consider it appropriate to make multiple statements hostile towards assisted dying while the review was underway?
Why did the AMA executive decide to continue to demand doctors not participate in assisted dying, when more than half of its own members said it could be appropriate clinical practice provided by doctors, nearly four in ten expressly disagreed with the policy, and a third said they’d participate if assisted dying were legalised?
Why does the AMA consider it appropriate to make repeated categorical, public statements that doctors should not be involved in assisted dying, when its Position Statement is not binding on its own members, let alone all Australian doctors?[1]
How can the AMA justify the incoherence of having an expressly opposed stance to assisted dying in its revised Position Statement while it remains totally silent on the matter in its Code of Ethics, revised at the same time?
How can the AMA legitimately demand to be centrally involved in developing an assisted dying framework — in which it says doctors should not be involved — for law reform, when it has no frameworks at all for the similar contexts of refusal of life-preserving medical treatment, continuous deep sedation until death, and the voluntary refusal of food and fluids (all currently lawful and practiced)? When will it develop and publish those?
Why does the AMA continue to present itself to the media and the public as representing all Australian doctors, when more than two thirds of them are not members?
Will the AMA include a formal analysis and critique of this deeply flawed policy review as part of its modernisation efforts in order to rebuild its brand value and stem the falling tide of its membership? That is, is the AMA prepared to learn from its mistakes?
[1] The AMA’s Code of Ethics is not binding even on its own members, either. So when the Code states “don’t engage in sexual, exploitative or other inappropriate relationships with your patients,” that’s merely a ‘suggestion’ or ‘recommendation’ rather than an ‘obligation’ as a member of the AMA.
Blog by Neil FrancisPosted on Friday 2nd December 2016 at 5:34pm
The AMA announces an 'update' of its "euthanasia and physician assisted suicide" policy.
The Australian Medical Association (AMA) executive (policy group) recently concluded a major review of its official policy on assisted dying. The last major review was in 2007. Through a deeply flawed process the AMA executive continues to expressly disrespect the diversity of views amongst Australian doctors — a diversity confirmed by its own review — and hasn’t altered its opposition to assisted dying in any meaningful way.
Unrepresentative of Australian doctors
The AMA promotes itself as “leading Australia’s doctors,” yet more than two thirds of Australian doctors (70.5%) are not members. Its executive might like to think it’s leading, but most Australian doctors aren’t following. Claimed representation is particularly important when it comes to professional medical practice policies, because the AMA behaves as though its policies apply to all Australian doctors.
So who did the AMA consult in conducting its major review of policy on assisted dying? Only its own members. In other words, the AMA claims to represent all Australian doctors, but in reality consulted less than a third of them in the setting of its assisted dying policy. As AMA member Dr Rosemary Jones pointed out, some doctors eschew the AMA because of its opposed stance towards assisted dying. That creates a sampling bias in the AMA’s study… against assisted dying.
Further, the response rate to its survey of members was around 13%, meaning that only the most engaged AMA members (thus around 4% of all Australian doctors) offered a voice.
Biased survey
There are numerous flaws in the AMA’s survey. Here’s just one. In the preamble to the questionnaire, the AMA expressly told responding doctors (who, remember, are AMA members and probably don’t want to tick off their association) what its positions on certain end-of-life practices were. Then, in the first questions, it asked the doctor whether they agreed with the positions: strategies certain to result in substantial confirmation and acquiescence biases.
This just isn’t on. As a professional social and market researcher, I sent a detailed critique of the many problems with the survey to AMA President Dr Michael Gannon. I received a courteous but dismissive response from administration. A highly-respected Fellow of the Australian Market & Social Research Society sent a similar critique, also receiving a non-committal reply.
Survey results
While the AMA hasn’t published the survey results in detail yet, key headline statistics have been reported. What did the AMA discover on the basis of a methodology swayed against assisted dying?
Around four out of ten doctors believe that doctors should be involved in assisted dying cases, while around five out of ten thought they shouldn’t. One out of ten had no view either way.
If assisted dying were legalised, a majority said that doctors should be the ones to do this work.
That’s a clear message that a substantial proportion of doctors think assisted dying can not only be legitimate practice, but is the business of the medical profession — at least for those who wish to participate.
Executive’s ‘interpretation’
And what did the AMA executive make of these important insights after deliberating on them for months? Here are the AMA’s previous and ‘revised’ core policy statements:
Previous (2007) statement
‘Revised’ (2016) statement
“The AMA believes that medical practitioners should not be involved in interventions that have as their primary intention the ending of a person's life. This does not include the discontinuation of futile treatment.”
“The AMA believes that doctors should not be involved in interventions that have as their primary intention the ending of a person’s life. This does not include the discontinuation of treatments that are of no medical benefit to a dying patient.”
Despite the gratuitous change of a few words after a year of ‘research,’ the statement remains the same.
Doctors and the public have a right to ask of the AMA, “what part of the evidence that there is a genuine diversity of respectable views, did you miss?”
Failure to respect diversity
The executive might argue that it did listen. Here are its statements about diversity:
Previous (2007) statement
‘Revised’ (2016) statement
“The AMA recognises that there are divergent views regarding euthanasia and physician-assisted suicide.”
“The AMA recognises there are divergent views within the medical profession and the broader community in relation to euthanasia and physician assisted suicide.”
Despite another increase in wordiness, this statement too remains the same.
The AMA executive says it recognises that there are divergent views, but by continuing to insist that no doctor should be involved in assisted dying, it reveals that it doesn’t respect some views. How does it justify this hubris?
Failure to respect the patient
The revised policy also says in part:
“Doctors should … endeavour to uphold the patient’s values, preferences and goals of care.”
The sting in the policy tail is, given the AMA executive’s wholly opposed stance toward assisted dying, that the doctor should only uphold patient values, preferences and goals of care if the AMA executive approves of them (and assuming to do so is legal).
Was it a foregone conclusion?
The AMA executive’s continued opposition to assisted dying was unsurprising. The signals were clear. While the policy review was in play, AMA President Dr Michael Gannon made a series of tweets and media comments, all unsupportive of or directly opposed to assisted dying. Here’s a few.
In response to an article in The Australian “Catholic stance allows eased exit”, he tweeted a faux ‘competition’ between palliative care and assisted dying:
@amapresident 13 Aug 2016: Different views society on assisted dying. Hope all agree improved PalliativeCare access a priority @westaustralian
He also tweeted in support of the ‘doctrine of double effect’, a controversial policy (which the AMA promotes as uncontroversial) that contends it’s quite OK for a doctor to hasten a patient’s death after all… provided they don’t really mean to: hardly a robust or verifiable standard.
@amapresident 24 Aug 2016: Doctors should be careful, must obey the law and understand their code of #ethics. Double effect is not #Euthanasia
In an article in The Australian on 15th September, Dr Gannon argued against assisted dying on the basis of it being ‘extremely complex.’ If complexity were a reason to oppose anything, the AMA would be opposed to the entire healthcare system: it’s incredibly complex. His argument collapses at the slightest inspection.
@amapresident 18 Sep 2016: Hippocratic medicine older than some of the world’s great religions, every political ideology, trend #ethics @medwma
Dr Gannon then invoked the Hippocratic Oath, which bans assisted dying. That’s cherry-picking at its best. Doctors do not take the Hippocratic Oath: it swears allegiance to ancient Greek gods, forbids women from entering the profession and outlaws surgery, amongst other things.
@amapresident 19 Sep 2016: Agree @DrSallyCockburn admire #euthanasia work done by @CMA_Docs. Equally careful, compassionate, intelligent approach from @TheBMA #ethics
He commends the British Medical Association’s “intelligent approach” against assisted dying: an approach I have comprehensively exposed as superficial and ill-informed fear-mongering, fiction, flip-flop and hubris.
@amapresident 1 Oct 2016: It is inevitable that if #Euthanasia laws are passed, they will over time be expanded to include children, mentally ill, vulnerable #ethic
Dr Gannon demonstrated ignorance of basic facts with this ‘slippery slope’ claim. In Oregon, which has the world’s oldest specific assisted dying framework (in effect since 1997), there have been no changes in who may qualify. He also ignores peer-reviewed research showing no ‘slippery slope’ for the supposed ‘vulnerable’. Canadian Professor Harvey Chochinov, Chair of his government’s expert panel which investigated legislative options for assisted dying, confirmed the evidential absence of the ‘slippery slope’ in a keynote address at Swinburne University in Melbourne last week.
@amapresident 11 Nov 2016: Doctors maintain this Trust with everyday care for patients, by upholding #DeclarationOfGeneva @medwma @juliamedew @Rania_Spooner #ethics
Dr Gannon also claimed that assisted dying would erode patient trust in doctors, at odds with the fact that people’s trust in doctors is high amongst OECD countries with assisted dying laws. Indeed, trust in doctors amongst Dutch, Belgian and Swiss citizens is significantly higher than Australians’ trust in our own doctors.
During the review period, Dr Gannon also repeatedly promoted the (medical) Declaration of Geneva (e.g. see previous tweet), which states that doctors must not participate in assisted dying. If the Declaration’s canonical opposition was indeed the authoritative stance on assisted dying, then it would be irrelevant for the AMA to conduct a review process of its policy.
Doctors and the public might ask a legitimate question: “Why did the AMA President think it appropriate to publicly and repeatedly indicate what review conclusion he favoured, while the review was in progress?”
Declining to correct misinformation
In September, the Medical Journal of Australia (MJA: a wholly-owned subsidiary of the AMA), published a news report containing significant misinformation that painted a hostile picture about assisted dying in Belgium. I published a critique of why the opinion was wrong, and commented on the online MJA article with a link to my correction. The MJA promptly deleted my comment.
AMA member Dr Rosemary Jones then put up the same objection which, by dint of her membership, they wouldn’t delete. The MJA then responded, but only to dig in its heels to defend the misinformation and reveal even more serious flaws in its arguments.
I wrote a further research-backed analysis of why its defensive arguments were even more wrong than the original and posted a note and link on the original MJA article page (Figure 1).
Figure 1: The second post on MJA inSight which was subsequently deleted.
Once again, my post has been deleted. The result of this is that erroneous information about Belgium remains published on the MJA website as though it is correct, while failing to mention or acknowledge that it has been soundly refuted.
It’s disappointing that the AMA and its President continue to make such uninformed remarks given that Dr Gannon claims to be a stickler for scientific evidence:
@amapresident 18 Aug 2016: Being a doctor is a huge privilege. Also carries responsibility to provide accurate scientific info, act ethically.
Spotlight on the AMA
Legitimate questions serve to shine a spotlight on the AMA. Firstly, given the circumstances, what was the likelihood of a real change to the AMA’s entrenched opposition toward doctor participation in assisted dying?
Secondly, given the AMA’s entrenched opposition, how can it expect its demands that it be consulted about any potential law reform to be treated seriously? If assisted dying is nothing to do with doctors, why is what doctors think relevant?
Utterly resistant to modernisation?
At its 2016 AGM, AMA member Dr Harry Hemley noted that the AMA largely represented its more hard-core, long-term older members and warned of the AMA’s increasing irrelevance and impotence (Figure 2). He moved an urgency motion to commission a review and report with “recommendations for a plan, vision and determination that will lead to re-invigorating and sustaining the AMA.”
Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform
The motion wasn’t in relation to an actual or particular reform: merely to investigate the potential for reform and to provide recommendations for consideration. We can only hope that the AMA will drag itself into the 21st century at some stage.
Conclusion
The AMA is deeply out of touch with Australians on the issue of assisted dying. It represents fewer than a third of Australian doctors and has failed to respect the very range of perspectives it obtained by consulting its members. It further strains its credibility by insisting that doctors mustn’t be involved in assisted dying, yet demanding to be consulted on any law reform to permit it.
If the AMA is to become relevant to contemporary society it must move on from the ‘old boy’ approach to medicine and adopt a stance of neutrality toward assisted dying. Only neutrality demonstrates appropriate respect for the true range of views held in good conscience by Australian doctors.
The AMA fails to represent the breadth of physicians perspectives around assisted dying.
This informative Go Gentle Australia video explains why the Australian Medical Association is out of touch with the wider Australian doctor community. Around a third of Australian doctors are members of the AMA.
The AMA currently holds a position of hostility towards assisted dying law reform, as it did against abortion before that was formally legalised. The doctors in this video explain how the AMA does not represent their views on assisted dying in restricted circumstances.
Blog by Neil FrancisPosted on Sunday 26th June 2016 at 2:05am
Schadenberg and Russell falsely call the Oregon Medical Association the "assisted suicide lobby" in contradiction of the facts.
Last week, Alex Schadenberg wrote—and Paul Russell republished—another nonsense article, this time about medical associations going neutral on assisted dying. They opine that there is no such thing as neutrality. And start out by getting their facts wrong... again.
Got the facts wrong yet again, lads
Messers Schadenberg and Russell claim that the Oregon Medical association is an "assisted suicide lobby" group. Had they bothered to check the rudimentary facts before sounding off, they would have known that the Oregon Medical Association remains neutral toward assisted dying. It reconfirmed its neutral stance as recently as early this month. It does not hold a 'supportive' stance.
How did Schadenberg and Russell come to their conclusion?
American Medical Association AGM
They refer to a motion that the Oregon Medical Association put to the recent annual general meeting of the American Medical Association. The motion sought to establish a process by which the American Medical Association would consult in order to re-evaluate its opposed stance to assisted dying, given that assisted dying is legal in a number of USA States and there are already many doctors who in good conscience provide assistance to die to qualifying patients.
Heavy-handed partisanship
In their usual style of heavy-handed partisanship, Schadenberg and Russell describe the Oregon motion as the "assisted suicide lobby" applying "pressure" to the American Medical Association.
They fail to level the same criticism at another group, the Louisiana Medical Society who put another motion to the meeting. The Louisiana motion sought to expressly confirm and entrench the American Medical Association's currently opposed stance. Schadenberg and Russell fail to criticize the Louisiana motion as "pressure," despite the fact that Oregon's motion was for open consultation, while Louisiana's was for a closed position.
Good sense prevails
In fact, they don't mention the Louisiana motion at all. Why? Because wiser heads prevailed at the national conference. The Louisiana motion was defeated and the Oregon motion was passed as I reported last week.
Desperate hyperbole
Schadenberg and Russell then desperately argue that you can only support or oppose assisted dying. There is no neutral, they say.
In the language of 'influence' we call this rhetoric "the sucker's choice." You put up just two options and demand folks pick one or the other.
"You're either for us or agin us!"
No other options, no nuances, no consideration of different options for different folks. Hardly the kind of stuff that would pass even a junior high school debate.
Back to the real world
Of course it's possible to be neutral.
Individually, a doctor may be personally opposed to assisted dying, but appreciate that another doctor, having equally examined their conscience, may support choice. Thus, the first doctor opposes for themselves but remains neutral to the position of other doctors. Indeed, an individual doctor may neither support nor oppose choice.
Collectively, it makes sense for a professional medical body to hold a neutral stance. How can it justify respecting the deeply-held beliefs and values of some of its members at the same time as explicitly disrespecting other members' views that are as closely examined and deeply held?
Conclusion
The best that opponents running the global charge against assisted dying can do is to first get their facts wrong (again), develop their false assumptions into shrill hyperbole, and then try to press the false dichotomy of a "suckers choice" into doing some heavy lifting: an exercise that falls flat on its face.
The evidence is crystal clear: they provide no real argument at all.
News reportPosted on Thursday 16th June 2016 at 12:18am
The American Medical Association has passed a resolution to re-examine its opposed stance to assisted dying.
During the professional meeting, the Louisiana State Medical Society introduced a motion to reaffirm the American Medical Association's policy against assisted dying. The motion was lost.
Instead, a motion callling on further study to examine the possibility of adpoting a neutral position on assisted dying was passed. The American Medical Association's Council on Ethical and Judicial Affairs will investigate and report back at next year's annual meeting.
The American Academy of Hospice and Palliative Medicine adopted a position of studied neutrality in 2007, so the American Medical Association has some catching up to do.
It remains to be seen if the Australian Medical Association's investigation into moving to a stance of 'studied neutrality' will succeed, bringing it into the modern era in which eight out of ten Australians believe the option should be available in restricted circumstances.
Blog by Neil FrancisPosted on Thursday 17th September 2015 at 6:06am
On 16th September 2015, the Victorian Director of the Australian Christian Lobby (ACL), Dan Flynn, appeared as a witness to the Victorian Parliament’s end of life choices inquiry being conducted by the Legal and Social Issues Committee. He made a number of mistaken statements, but what was most worrisome was the revelation of the ACL’s real agenda: to wind back patient rights more than a quarter century.
In his opening address, Mr Flynn opined that assisted dying was 'not supported' by a 'broad base' of Victorian Christians (not just the ACL). This belief is diametrically at odds with clear and repeated evidence from multiple sources.
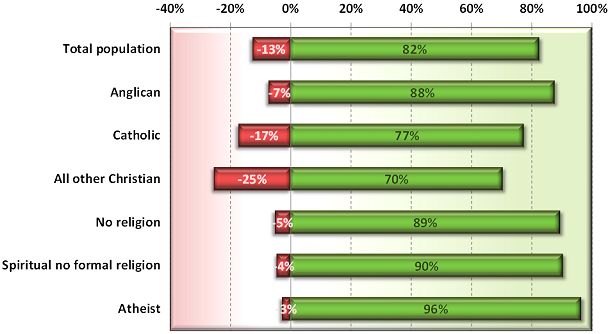
In 2012, I reported on a Newspoll study into Australian attitudes towards assisted dying. Not only did a whopping majority of citizens support assisted dying, but so did a great majority of Anglicans, Catholics and other Christians (Francis 2012).
Newspoll 2012: Australian attitudes to assisted dying law reform by religion (green=support, red=oppose)
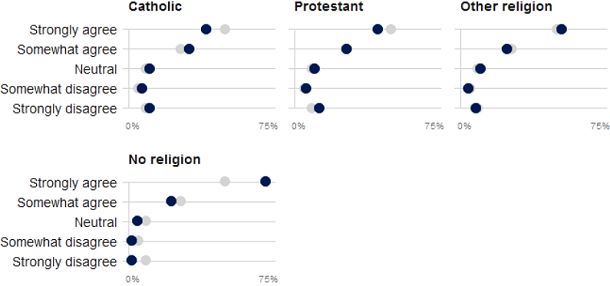
These national results are reflected by a sample of over 60,000 Victorians through the VoteCompass system during the 2014 Victorian election (Stayner 2014). It confirms a substantial majority of Catholics, Protestants, other religious and non-religious Victorians support assisted dying law reform.
VoteCompass 2014: Victorian attitudes to assisted dying law reform by religion (grey=population average)
Out of date
Mr Flynn then referred to a Tasmanian Parliament’s inquiry into assisted dying which rejected law reform. However, the inquiry to which he refers was held in 1998, when Oregon’s Death With Dignity Act had barely been established, the Northern Territory’s Rights of the Terminally Ill Act had been extinguished within just eight months of coming into operation, and the Dutch, Belgian, Luxembourg, Washington and other legislation and judgements did not yet exist.
So, the Tasmanian Parliament’s rejection came from a position of a then general lack of information. The Oregon law has been in effect since 1997, the Netherlands and Belgium since 2002, Washington since 2008, Luxembourg since 2009, and so on. There is now plenty of evidence that assisted dying law reform doesn’t cause slippery slopes that opponents love to theorise about.
Wrong about ‘United Nations’
Mr Flynn then said that the United Nations had in 2012 expressed concern about a ‘lax attitude’ towards euthanasia in Europe, specifically mentioning the Netherlands and Belgium. This is completely untrue. Because it’s easy to make a simple blooper during a presentation, we’ll put aside the fact that he meant to refer to a completely different organisation: the Council of Europe.
We know this because he read directly from Council of Europe declaration 1859 (Council of Europe Parliamentary Assembly 2012). His ACL submission (Australian Christian Lobby 2015) reports (as he read out) exactly one sentence of the declaration, with his added emphasis, as:
"Euthanasia, in the sense of the intentional killing by act or omission of a dependent human being for his or her alleged benefit, must always be prohibited."
But presented in this manner the statement is quite misleading. As I explain in a forensic analysis of the misinformation campaign about this resolution (Francis 2015), the resolution was utterly clear about its intent: it was not about euthanasia (it explicitly said so), but rather about advance care planning. What the resolution spoke against (in the one sentence conveyed above) is non-voluntary euthanasia, not voluntary euthanasia. Both sides of the assisted dying debate agree that non-voluntary euthanasia (one person deciding for a hastened death on behalf of another) is not acceptable. It is not contentious.
In no way did the Council of Europe's resolution critique voluntary euthanasia or comment on any jurisdiction in which it is legal. And, the United Nations source to which the ACL submission refers was released in 2001, fourteen years ago and at the time of the Netherlands' Euthanasia Act was before the Dutch Parliament. With then limited information about how such laws work in practice, it expressed concern about the upcoming Act.
Wrong about Belgium’s law and practice
Mr Flynn referred vaguely to two cases of euthanasia in Belgium in which persons who requested and received euthanasia were not experiencing intolerable pain, which Mr Flynn asserted was a required safeguard in Belgium’s euthanasia Act. This was another supposed example of transgression of safeguards. Wrong again.
While the Belgian Euthanasia Act is officially published only in Dutch and French, a robust English translation has been prepared under the supervision of Professor Herman Nys of the Centre for Biomedical Ethics and Law at the Catholic University of Leuven (see Parliament of Belgium 2002). The word ‘pain’ does not appear in the Act… at all. What does the Act have to say about the legislature’s intent on who may qualify? The relevant clause in Section 1 says:
— "the patient is in a medically futile condition of constant and unbearable physical or mental suffering that can not be alleviated, resulting from a serious and incurable disorder caused by illness or accident."
It’s abundantly clear: mental suffering from an illness or accident qualifies as much as physical suffering, and the suffering does not need to be ‘pain’ as Mr Flynn mistakenly asserted to the Parliamentary Committee.
Mr Flynn also stated that there are mobile end-of-life units in Belgium. There aren’t. (But there are in the Netherlands, and they must follow precisely all the same requirements as anyone else. They operate to provide choice to patients whose regular or reachable doctors disagree with assisted dying and therefore decline to evaluate whether the patient may qualify under the Act.)
Confused about Advance Care Directives
In further testimony, Mr Flynn opined that the degree to which a doctor should be allowed to override a patient’s Advance Care Directive (ACD) is in part influenced by whether the doctor can speak with the patient.
But if the patient can currently speak and participate in decision-making, the advance care directive doesn’t apply: it is mute and of no effect. An ACD only applies when the patient cannot currently participate in their own decision making. That’s (only) what it’s for.
Winding rights back more than a quarter century
But the most worrying aspect Mr Flynn’s testimony was the revelation of ACL’s opposition to the right to refuse unwanted medical treatment.
The Medical Treatment Act 1998 (Vic) has enshrined for now more than twenty five years a patient’s right to refuse any unwanted medical treatments. In 2003 the Supreme Court of Victoria determined that artificial nutrition and hydration (i.e. via tubes) is medical treatment and can therefore be refused under the Act.
But Mr Flynn repeatedly argued that withholding or withdrawing artificial nutrition and hydration, if the patient’s body could ‘absorb’ them, could amount to physician-assisted suicide, and that doctors must be allowed to override refusals. On the matter of patient autonomy, he said that some autonomy rests "with the patients, but a lot of the autonomy in fact is with the doctor”.
When asked if a Jehovah's Witness who refuses a life-saving and simple blood transfusion ought to be allowed to do so, he conceded that they should be entitled to, but that such a case was a “bit of an outlier”. He didn’t explain on what moral grounds one person could refuse a simple procedure to save their life, but another person mustn’t be allowed to even if the likelihood of saving life was doubtful.
So, the ACL’s real agenda is revealed: it recommends winding back the legislative clock more than a quarter century so as to force patients to endure some medical interventions that they don’t want and firmly refuse, if the doctor wishes to proceed.
No wonder the Committee repeatedly questioned Mr Flynn to ensure they had heard and understood his testimony correctly. In conclusion, Committee Chair Edward O’Donohue observed that Mr Flynn’s evidence was “quite surprising” and “quite contrary” to wide evidence already given.
And it’s no wonder that Theo Mackaay, General Secretary of the Victorian Council of Churches—a group of 30 member churches representing mainstream Christianity—criticised the ACL as “fundamentally conservative” and expressed “deep concern that media portrayal of statements from an established and narrow focused lobby group is presented as being representative of the entire Christian community” (Uniting Church in Australia 2011).
-----
References
Australian Christian Lobby 2015, Submission to the Legal and Social Issues Committee on the Inquiry inito End of Life Choices, Parliament of Victoria, Melbourne, pp. 1-17.
Council of Europe Parliamentary Assembly 2012, Resolution 1859 (2012): Protecting human rights and dignity by taking into account previously expressed wishes of patients, Europe, 25 Jan, pp. 2.
Francis, N 2012, Australian public desire for legalisation of assisted dying in restricted circumstances, YourLastRight.com, Melbourne, pp. 11.
Parliament of Belgium 2002, 'The Belgian Act on Euthanasia of May 28th 2002 (unofficial English translation)', Ethical Perspectives, vol. 9, no. 2-3, pp. 182-188.
Uniting Church in Australia 2011, Australian Christian Lobby does not represent all Australian Christians, nor all Christian viewpoints, 8 Dec, Media Room, viewed 11 Dec 2011, <http://blogs.victas.uca.org.au/mediaroom/?p=971>.



 Infographic summary of 'AMA uncovered'
Infographic summary of 'AMA uncovered'
 @amapresident 13 Aug 2016: Different views society on assisted dying. Hope all agree improved PalliativeCare access a priority @westaustralian
@amapresident 13 Aug 2016: Different views society on assisted dying. Hope all agree improved PalliativeCare access a priority @westaustralian Figure 1: The second post on
Figure 1: The second post on  Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform
Figure 2: Dr Harry Hemley speaks to the urgency motion to investigate organisational reform