Blog by Neil FrancisPosted on Wednesday 26th May 2021 at 4:03am
A new book of anti-VAD polemical anecdotes, published by Springer
The other day a TV commercial from more than 30 years ago popped into my head. It was a humorous slice-of-life scene in which a teenage son gobbles down a breakfast bowl of Sultana Bran cereal. He complains that his health-kick girlfriend had made him eat vegetarian the night before. His family eye each other with mirth as he eats.
The punch line? “Don’t mention it’s healthy and they’ll eat it by the boxful.”
The Kellogg's Sultana Bran TV commercial from 1990.
Despite having worked in advertising research for years, I’m sure I hadn’t thought of this ad for at least a couple of decades. So what brought this vignette suddenly to mind?
It was the release of a new book by academic publisher, Springer: Devos, T, (Ed.) 2021, Euthanasia: Searching for the Full Story - Experiences and Insights of Belgian Doctors and Nurses, Springer, Leuven.
How terrific to have a new academic tome on the Belgian voluntary assisted dying (VAD) experience, I thought, as I downloaded the eBook version.
But then…
Imagine my surprise and disappointment then, to discover this is no scholarly tome with ethics-committee-approved study methodologies, carefully cited and transparent sources whose authenticity and veracity could be checked by anyone with a smidgin of scholarly acumen.
No, the kindest description I can give this blancmange of offenses is… a series of “essays” all singing from the same hymn sheet. More on that shortly.
The book launches into — let’s not beat about the bush — bullshit from the get go. In the Foreword, Jacques Ricot invokes the Hippocratic Oath as a still-relevant “religious standard”. Oh dear. You mean that oath that prohibits surgery, prevents women from entering the profession, and swears allegiance to ancient Greek gods?
He then goes on to describe VAD as a “desperate act of two people [the doctor and patient] trapped by helplessness.” He invokes cracks opening up in sea walls and waves that can only widen them. There’s your horizontal oceanic equivalent of the inevitable “slippery slope”.
Helpfully, he forewarns that all the authors in the book “do not believe that euthanasia can be a medical or a caring act.” OK, so not a range of views, then.
He also refers to the authors as “resistance fighters”, giving a heads-up that these writers feel they’re losing the battle.
And yet more
Then, anti-VAD campaigner Margaret Somerville repeats her rubbish claims that legalised VAD leads to suicide contagion. I’ve repeatedly taken Somerville to task over her serial misinformation, as well as noting the latest evidence from Switzerland which VAD opponents never mention… for a reason.
Somerville repeats yet again her refrain that “the case against [versus for] euthanasia is much more difficult to promote … because it is more complex”. No, it isn’t. It’s just that the majority now no longer take conservative religious doctrine as … shall we say, “gospel”. That’s especially true when her strongest ambit is to appeal to “a human way of knowing” (without mentioning her hobby horse, “moral intuition”, by name), and expressly noting that the stories that follow are not based on the usual scientific standards of evidence.
And there you have it. A series of “essays” by persons ideologically opposed to VAD, adorned with numerous uncheckable anecdotes and tawdry claims, appeals to slippery slopes, misrepresentation of data such as the non-voluntary euthanasia rate in Belgium, “intuitive” claims that the bereaved suffer as badly from lawful VAD as do families of those who have suicided violently and alone (despite multiple peer-reviewed studies showing VAD bereaved cope well). The list goes on.
Who are these people?
This of course begs the question: who are these people putting themselves forward as experts in VAD? Remember, these are people claiming expertise in a subject they’ve never participated in, and swear they never will. No doubt they are indeed experts in their own individual disciplines. But not in VAD.
It’s like asking (only) a bunch of hardened atheists to write an authoritative book on Christian spirituality.
Well, many of the names are already well-known in VAD (and especially anti-VAD) circles. Others took a bit of research to track down. Much of the work for the following backgrounders was accomplished by my friend the talented Chrys Stevenson. We compared notes.
The point of the research was not to attempt an inappropriate ad hominem attack. Without attempting to bore, I’ve already given a host of reasons as to why the quality of the essays in this book are very low. No, the point is to find common influences and agendas as to why that might be.
So lean in, dear reader, here we go. And to aid comprehension, may I suggest that you watch for the words in bold?
The editor — Timothy Devos
Timothy Devos is a Professor of Medicine (haematology) at Catholic University Leuven. He is a past president of the Medicine and Dignity of Man Association, an apostolate of the Catholic Regnum Christi movement, which believes that “the positions adopted by the Catholic Church in matters of bioethics are good, prudent”.
Foreword 1 — Jacques Ricot
Jacques Ricot is an Associate Researcher at Nantes University in France. In a 2003 paper he argues that secular philosophy needs to draw on the religious understanding of forgiveness. In 2014 he attended a conference on “dying with dignity” at the Catholic Notre Dame, Paris, articulating views harmonious with Catholic doctrine. In 2018, the European Federation of Catholic Doctors Associations and the Catholic Centre of French Doctors thanked him for valuable contributions to their thinking about human medicine.
Foreword 2 — Margaret Somerville
Professor of Bioethics at the (Catholic) University of Notre Dame Australia. (This is curious given that her CV mentions no earned tertiary qualification in either ethics or philosophy.) Somerville is a loyal Catholic who has for years been given pre-eminent position regarding Catholic bioethics above even the church itself at the L.J. Goody Bioethics Centre, as I’ve pointed out before.
The L.J. Goody Bioethics Centre is run by the Catholic Archdiocese of Perth. The Catholic Archbishops of Perth and Sydney are the ultimate controllers of the University of Notre Dame Australia.
Foreword 2 — Wesley Ely
Dr Wesley Ely is a Professor of Medicine at Vanderbilt University Medical Centre in Nashville, Tennessee. He is President of the Nashville Guild of the Catholic Medical Association. He has given numerous addresses from a Catholic perspective on topics such as “Preaching the gospel through service”, “Five principles of service in living the gospel”, “Deepening our prayer life”, “Viaticum: lessons learned from dying patients seeking our Lord”, “Top 10 tips at the heart of Christian discernment” and “A treatise on the true devotion to the blessed virgin by a lay doctor”.
Contributor — Eric Vermeer
Mr Vermeer is a nurse educator and the ordained Deacon of the Catholic diocese of Namur. His adopted son is also a Catholic priest. He is a past President of the European Institute of Bioethics, a group that claims to be independent and not of a religious nature, yet “attentive to religious traditions”. It lobbies for positions that are consistent with Vatican doctrine, such as against abortion and VAD. Quite a number of the Institute’s committees are known religious people, including some from the Catholic University of Leuven.
Mr Vermeer has recorded an anti-VAD video for ADF International, which runs the Arete Academy, a centre for religious academics based on “excellence and moral value”… at least according to their interpretation of the Bible.
Contributor — Catherine Dopchie
Dr Catherine Dopchie is an oncologist at the Centre Hospital of Wallonia. She told the Society for Religious Information Italy, published by the Catholic Press Agency, that “death is the enemy of mankind”, that “we have been created for life”, that “those who have met God in their lives, know that death is not the winner”, and that “every man is precious to God and that the entire life is sacred”.
Dr Dopchie has also recorded an anti-VAD video making unsubstantiated claims, for ADF International.
Contributor — Willem Lemmens
Having earned his doctorate at the Catholic University of Leuven, Professor Willem Lemmens is now Chair of the Department of Philosophy at the University of Antwerp. In 2018, Professor Lemmens argued against VAD at the (Catholic) Anscombe Bioethics Centre in the UK, and spoke with Catholic newspaper Crux, to spread the misinformation that Belgium’s law was originally only for terminal illness (it never was), and to complain that (Catholic) Belgian Brothers of Charity were now allowing VAD to occur in their healthcare facilities.
He also sits on the General Council of the University Centre Saint-Ignatius Antwerp, which was established by a Jesuit (Catholic) order, and whose purpose is to continue to promote Jesuit Christian ideology.
Contributor — An Haekens
Dr An Haekens was educated at the Catholic University Leuven. She is a psychiatrist and medical director at the (Catholic) Alexian Care Group in Tienen, Belgium. It was established by the (Catholic) Belgian Brothers of Charity and states that “we start from our own Christian identity” and “we want to keep alive and implement the spirituality of the Alexians”.
Dr Haekens writes periodically for Belgian Catholic magazine Tertio, including stating that she would never participate in VAD. In 2021 she was interviewed by Belgian Catholic radio station Radio Maria, having been awarded the annual prize for spiritual care by the Professional Association of Care Pastors, the association for Catholic chaplains.
She is married to Dr Didier Pollefeyt, Catholic Professor of Theology and Religious Studies at the Catholic University of Leuven. He is also an Honorary Professor at the Australian Catholic University.
Contributor — Rivka Karplus
Dr Rivka Karplus is a family physician and an internal medicine and infections specialist, based in Israel. In 2018 he attended a colloquium at the College des Bernardins in Paris — a Catholic theological and biblical studies centre — as a representative of the Jerusalem Kehilla, a congregation of Hebrew-speaking Catholics. He is warmly cited in a 2016 anti-VAD publication by the Catholic Caritas in Veritate Foundation, which attempts to provide representatives at the UN and other international organisations with Catholic, Christian “expertise and strategic thinking”.
Contributor — Marie Frings
Dr Marie Frings is a Brussells-based GP specialising in palliative care. She writes for Catholic group Consecrated Lives which promotes increasing evangelical commitments. In such an article in 2007, she cites the CatholicCongregation for the Doctrine of the Faith as an authority on end-of-life decisions, and notes that sometimes she felt uncomfortable that patients would have their arms tied to be force-fed against their wishes so they lived indefinitely. She firmed her views that tube feeding was not mandatory when it is an extraordinary measure, with the help of several Catholic theologians and the pro-life committee of the episcopal conference of American (Catholic) Bishops.
She argued “respecting the conscience of others” in this regard, yet expressly rejects such conscience when it comes to choosing a peaceful, hastened death by VAD.
Contributor — Benoit Beuselinck
Dr Benoit Beuselinck graduated from the Catholic University of Leuven in Belgium, and has for years worked in the university’s hospitals. In 2017 he spoke at an anti-VAD conference at the Catholic Anscombe Bioethics Centre in the UK.
In an article in the Catholic magazine Logia, he claims that “proper palliative care makes assisted dying unnecessary”, even though it is well-established that this isn’t true.
He alleges in the Catholic Herald that Belgian nurses and social workers are quitting their jobs because palliative care units are being turned into “houses of euthanasia”, and that doctors in palliative care units “have to euthanise patients”. He also claims that some patients are afraid to go to hospital in case they are either coerced into euthanasia or are deliberately killed without their consent. This is a perversion of the original Netherlands accusation by the Vatican, which itself was entirely false.
Dr Beuselinck has also made an anti-VAD video for ADF International, making unsubstantiated claims that “doctors hide behind their patients’ wishes”, “supply creates demand”, “the doctor has his back to the wall”, “we want euthanasia for everyone”, “doctors who prefer not to do it are not respected”. He cherry-picks Belgian non-voluntary euthanasia data to wrongly make the case that their VAD law has caused (or at least worsened) that practice; the opposite of the truth. He says that euthanasia is an act against nature, opens the floodgates, that we no longer favour the love we show in taking care of someone, and that the depressed may now think “if the doctor can kill, then what is my life worth?”
Contributor — Julie Blanchard
Dr Julie Blanchard is a French-trained GP who specialises in palliative care. She works at the Catholic University of Leuven’s second hospital, in Namur, and never participates in VAD. Contrary to Dr Beuselinck’s claims that palliative care workers opposed to VAD are disrespected and forced to participate, Dr Blanchard reports that other doctors respect her opposition, and that VAD teams take care to ensure those who are against VAD are not present at the time of a lethal injection.
It's astonishing how inconsistencies like this — those opposing VAD are respected but are not respected — reduce the book’s coherence.
Contributor — François Trufin
François Trufin is an emergency nurse at St Nikolaus Hospital in Eupen, Belgium. The hospital was founded and continues to be sponsored by the Catholic church, “continuing [the] obligation of the founders” for a “Christian worldview”.
Religious petticoats and the Catholic Communicator’s Guild
So there you have it: the Catholic connections of the people involved in the production of this risible nonsense, which brims with innuendo, arguments and misinformation consistent with those of the Catholic church and other Catholic apologists.
I’ve written before how Catholic Archbishop Anthony Fisher has expressly argued for organising a line-up of sympathetic (i.e. Catholic) doctors, lawyers and others to put such information about, and yet, how they hide their religious petticoats while doing so. I’ve further exposed a network of Catholics who promote the church’s line on VAD — a network I call the Catholic Communicator’s Guild.
This book furnishes an international example of the same principle: a group of Catholics promoting entrenched church lines on VAD, but hiding their religious petticoats all the while.
You may wonder how many times the word “Catholic” appears in said book. The answer is: exactly zero. And mentions of “religion” and “faith” appear as abstract and conceptual argument, e.g. if a person of faith…
Not the first time it’s been published
But a further issue arises in respect of this book: it’s not the first time it’s been published. It was published two years ago by Mols Editions (Wavre) under the title Euthanasia: Behind the Scenes — Reflections and Experiences of Caregivers. Tellingly, it was published in French and mentions the French parliament grappling with VAD law reform. (The current French VAD Bill, which appears to be supported by a majority of MPs, has been filibustered with well over 2,000 (two thousand) amendments submitted by just five MPs.)
Unlike the original which you have to buy, this Springer version is “Open Access”, meaning you can download the book from the publisher for free. So is this further edition vanity publishing?
The reason I ask is that Springer Publishing is owned by Springer Nature. That’s a company whose purpose is to make money for its owners via academic publishing. So publications have to be paid for either by sales, or by authors. Since there are no sales, the authors (or someone on their behalf) will have had to pay for the book.
According to their fee schedule, Springercharge US$15k (around AUD$20k) plus taxes for publishing a tome of this nature.
So: who paid for the book?
Conclusion
Far from a carefully researched collection of studies into VAD practice in Belgium, this polemical book relies heavily on the “moral intuitions” of innuendo, unverified anecdote and misinformation. It’s consistent with the propaganda put about by the Catholic church, yet not once throughout the entire book does anyone mention their deep Catholic connections. Indeed, you could be forgiven for thinking they’d taken some care to cover their religious petticoats.
A serious compendium of proper, scholarly studies of VAD practice, good and bad, is always welcome. This book is not it.
In my view, the tome does no favours for Springer, which has a solid reputation for academic and scholarly publication.
And, back to that 1990 TV commercial for boxes of breakfast cereal. It had popped into my head as an analogue: “Don’t mention it’s religious and they’ll publish it by the book-full.”
Blog by Neil FrancisPosted on Thursday 23rd May 2019 at 2:39am
Palliative care specialist advances incoherent reasons to oppose VAD.
Director of Palliative Care at Cabrini Health, Associate Professor Natasha Michael, yesterday published an opinion piece in The Age newspaper. In it, she rails against Victoria’s voluntary assisted dying (VAD) Act which comes into effect on 19th June. Instead she articulates an arrogant and prescriptive view of what Australians should and shouldn’t be allowed, consistent with Catholic dogma, as I uncover.
Michael, along with fellow devout Catholic Dr Stephen Parnis, ‘tirelessly’ opposed the introduction of Victoria’s VAD law. They continue to actively oppose it, and her opinion piece reveals her spurious ‘reasoning’.
The Catholic Healthcare brick wall
More than half of all palliative care services in Australia are delivered through Catholic institutions, of which Cabrini Health is one arm. These institutions have determined that VAD will not be available in any of their facilities or via any of their services, even if the individual patient and doctor are supportive.
This arbitrarily limits access to lawful choice by citizens.
Confected ‘institutional conscience’
I say ‘arbitrarily’ because ‘institutional conscience’ is a confection: it doesn’t really exist. Only real persons have conscience. The fabricated dictates of any institution — presented as ‘moral rules’ — extinguish the actual real conscience of those who exist within it: at least, those whose conscience differs.
The upshot is that a specific cohort of religious, celibate men in Rome dictate whether Australian citizens can or can’t obtain lawful healthcare services from half the service providers.
So let’s examine what the institutional ‘conscience’ has to say.
Disgraceful framing in headline
“We can’t let voluntary assisted dying negate our commitment to the ill”, Michael’s article headline screams.
Firstly, VAD is not available to the “ill”. It’s available only to those with terminal illness and intolerable suffering, according to 68 criteria.
Secondly, Michael invokes a false dichotomy of “negating a commitment”. VAD does not “negate a commitment”. Indeed, to fail to hear and respect a persistent, fully informed and tested request for VAD that meets all the criteria is to negate palliative care’s commitment to honour the patient’s deeply held values, beliefs and decisions.
Medical-coloured glasses
“The introduction of voluntary assisted dying legislation in Victoria on June 19 will remind us of the occasional failure of medicine,” Michael says.
That’s it. The patient’s death is a failure of medicine, as though a person’s death is a medical event rather than a deeply human and private one of personhood.
It also flags the common but immature medical assumption that “death = failure”. Death is inevitable, not a “failure”. The key question about death for people with terminal illness is “how”, and Michael presumes to prescribe the “how”: being receptacles for interventions that she and her colleagues provide.
Let’s be clear. Many people are helped enormously by palliative care. That’s a great credit to the discipline’s specialists.
However, as Palliative Care Australia acknowledges, even the best palliative care can’t relieve all excruciating, debilitating and humiliating refractory symptoms.
Michael’s answer to this sometimes “failure” of medical interventions? Deliver more interventions, whether the patient considers them consistent with his own values, beliefs and circumstances or not.
They’re very heavily medical-coloured glasses indeed.
Three faux ‘threats’
Michael then invokes three faux ‘threats’ supposedly caused by lawful VAD in Victoria.
Faux threat 1: “Validating suicide as an acceptable choice”.
Michael exposes her own bias here: that all self-hastening of deaths are the same — that there is no meaningful difference between a dying person who is fully informed and whose rational choice for a peaceful assisted death has been extensively tested, with the violent and impulsive action of a person suffering a temporary, resolvable personal crisis, be it mental illness, substance abuse, intimate relationship breakdown or other circumstance.
Michael is pretty much on her own here. Most Australian doctors make a clear distinction between these very different contexts.
Faux threat 2: “accepting substandard medical care by supporting the lack of rigour in defining [VAD] eligibility”.
Michael overlooks that there is a major lack of rigour in existing, lawful end-of-life choices.
There are no statutory requirements for a patient to refuse medical treatment, even if the treatment would be life-saving.
There are no statutory requirements for the voluntary refusal of food and fluids in order to die, either.
More critically, despite terminal sedation being a common end-of-life medical practice but ethically problematic (including that it may hasten death and may not alleviate intractable symptoms), not only is there no statutory requirement for its practice, but neither the Australian Medical Association nor Palliative Care Australia have official guidelines on its practice.
Thus, in railing against the staggering 68 standards of practice prescribed in Victoria’s VAD law — vastly more than any other in the world — as a “lack of rigour”, Michael makes no mention of three other major life-end choices that have no such standards, including her own discipline’s terminal sedation.
Doctor, heal thyself (and thine own systems).
Faux threat 3: “introducing into the healthcare curriculum the intentional ending of life as acceptable medical treatment”
Michael creates a misleading impression here. By referring to ‘curriculum’ you might think that all medical students would have to undergo training on how to end lives, or be ‘indoctrinated’ to accept VAD. That is not true.
To be able to prescribe lethal medication under Victoria’s legislation, the doctor must undergo additional training in relation to that procedure. Doctors will only receive the training if they self-nominate for it: it’s not compulsory.
If, by ‘curriculum’ Michael means only “VAD might be discussed” in medical school, then she would have to articulate why termination of pregnancy (to which the Catholic church objects) should not be discussed, either. Nor the transfusion of blood, since many Jehovah’s Witnesses object to the procedure.
Own failure in palliative care principles
Nowhere in her opinion piece does Michael acknowledge that the patient may deeply hold values and beliefs that validly favour VAD. Thus, Michael offends the first principle of palliative care which is to make the patient the centre of care and to honour as much as possible the patient’s values, beliefs, attitudes and wishes.
Indeed, in her conclusion, Michael states that palliative care “remains committed to the ongoing accompaniment of our patients. Not abandoning them” and which is “the only plausible method of compassion and care.”
This surely is the most egregious and arrogant self-interest of all: patients must subject themselves to being accompanied by palliative care staff and their ‘interventions’ whether they want more or not.
On the contrary, to fail to hear and respect a genuine, informed and persistent request for a peaceful hastened death from a dying patient for whom this accords most firmly with his deeply held values and beliefs, is to abandon the patient.
Conclusion
Michael is of course entitled to her personal stance, and I celebrate her right to hold her views: for herself.
However, her ‘requirement’ that all Victorians be denied access to an option that four out of five believe to be moral — and instead subject themselves to interventions administered by Michael and her colleagues — reveals an unattractive arrogance.
It’s a shame that Catholic bioethics doesn’t teach more about reflection, especially as to whether one’s own beliefs ought to dictate and limit the choices of others with equally firmly held, though different, values.
In the meantime, Victorians are pawns to the tyranny of the Vatican as to whether there is a local healthcare facility that will hear and examine their request for a peaceful, assisted death in the face of terminal illness.
Blog by Neil FrancisPosted on Monday 13th November 2017 at 6:28pm
The deeply-flawed Jones & Paton, and Kheriaty articles purporting to show suicide contagion.
In the ongoing political campaign against assisted dying law reform, opponents have spread one piece of egregious misinformation after another. One of the most common is supposed “suicide contagion” from assisted dying laws to general suicide, a theory popularised by Catholic Prof. Margaret Somerville. Despite the nonsense of her claim being comprehensively exposed, she still believes that her opinion “will prove to be correct.” Two journal papers published in 2015 purported to, but didn't, establish suicide contagion in Oregon and Washington states.
Assisted dying law reform opponents are still relying on a 2015 paper by Catholics David Jones and David Paton, bolstered by a glowing editorial of it written by Catholic psychiatrist Aaron Kheriaty, published in the Southern Medical Journal, as continued ‘proof’ of suicide contagion theory, at least in respect of USA states Oregon and Washington (since data from other lawful jurisdictions contradicts the theory).
Jones & Paton’s article reported the use of econometric modelling to test for ‘suicide contagion’ from Oregon and Washington’s Death With Dignity Act (DWDA) laws. But, in an exposé to be published this week, no fewer than ten ‘deadly sins’ of the study are peeled back to reveal the rot within.
The very deep flaws and biases of the original articles include:
Cherry-picking information from cited sources to argue their case, while omitting information from the same sources that contradicted their case;
Including test and control subjects whose consequence was likely to maximise the likelihood of finding a positive association;
Demonstrating a poor understanding of suicide and its risk and protective factors and failing to control for most confounding effects in their econometric model ‘pudding’;
Overegging the “causative suicide contagion” interpretation when no correlation between assisted dying and general suicide rates was found; and
Failing to use direct, robust and readily-available evidence that showed their study couldn’t possibly have hoped to return scientifically valid “contagion” proof.
The USA’s National Violent Death Reporting System (NVDRS), of which Oregon is a founding member, shows that even if “assisted dying suicide contagion theory” were true, fewer than 2 of 855 Oregon “total suicides” in 2014 could have been attributed to “contagion” from DWDAs.
Further, both Oregon and Washington state rankings for suicide rates have improved, not deteriorated, since their DWDAs came into effect, while the suicide ranking for a relevant control state — Oklahoma — has deteriorated substantially over the same time.
Ultimately, through numerous and deep methodological flaws, the Jones, Paton and Kheriaty articles reveal a bias to promote “assisted dying suicide contagion theory” while ignoring the robust evidence from multiple lawful jurisdictions, including in their own ‘study,’ that contradict it.
The exposé, titled “The ten deadly sins of Jones, Paton and Kheriaty on ‘suicide contagion’,” will be published by DyingForChoice.com later in the week.
Blog by Neil FrancisPosted on Friday 13th October 2017 at 10:11am
The Guardian reports a fracas within the Anglican church over a $1m political expenditure.
Anglican and Catholic bishops seem to be going out of their way to alienate their constituencies, including in respect of voluntary assisted dying and marriage equality law reform. As a result, the writing on the wall is writ large for the continued decline of religion in Australia.
Many Australian clerics are trying their hardest to foil Parliamentary attempts to drag Australia into the 21st century on social policy. They seem to care little for the ongoing demise of their own constituencies.
Religion declining since the 1960s
Religious affiliation in Australia has been declining consistently since the 1960s, consecutive Australian Bureau of Statistics (ABS) census figures show (Figure 1). At the 2016 census, somewhat more than half (60%) of all Australians claimed a religion. More Australians than ever before identified as ‘no religion’ — for the first time ever a larger group than any single religious denomination.
Figure 1: Australian religious affiliation by census year Source: ABS
Weak religious commitment
Not only has religious affiliation been dropping, but the nature of the affiliation is weak (Figure 2). Amongst the two largest religious denominations, a quarter of Catholics (26%) and nearly half of Anglicans (47%) are Notionals: that is, they identify with the denomination but never attend religious services. More than half of Catholics (52%), and four in ten Anglicans (41%), attend religious services only occasionally (Occasionals: several times a year or less often).
Figure 2: Australian denominations and Australian religious identity (ARI-6) Source: Australian Election Study (AES) 2016
Just 22% of Catholics and a mere 12% of Anglicans demonstrate commitment to their denomination through dedicated service attendance (Regular = monthly or more often, and Devout = weekly or more often).
The picture is particularly grim for the Anglican church, dominant in Australia from Federation until the 1960s. With both a deeply impoverished affiliation rate in 2016 (13.3%), and just 12% of the flock dedicated to service attendance, a miniscule 1.6% of Australians are committed Anglicans.
The picture is only slightly better for the Catholic church. With 22.6% affiliation in 2016, and 22% of those committed to service attendance, it's a slightly larger but still damningly small 5.0% of Australians who are committed Catholics. Further, the Catholic church’s affiliation may be significantly lower at the next (2021) census, as Australians vent their dismay and disgust at how badly it’s handled the scourge of child sexual abuse that’s occurred under its ‘pastoral umbrella.’
Hollow ‘leadership’
Across all religious denominations, just 16% of Australians are committed to their denomination — Regular or Devout religious service attenders — while 30.1% Reject religion altogether.
And yet those at the head of their ships of faith still demand that we listen to and comply with their moral dictates, assuming that they have an automatic right to steer our morality in their own chosen direction. If they think they’re ‘leading,’ most Australians aren't following.
The indications are that they're going the way of Kodak, now a small, wan shadow of its former dominant self. If the Anglican and Catholic churches were companies with voting shareholders (or even not-for-profits with voting members), the Boards and executives (archbishops and bishops) would have been, for overseeing such profound and continuing erosion of their brand franchises, replaced long ago.
Entrenched rather than learning
You’d think all this would be a warning message to archbishops and bishops to seek to understand their flocks and build bridges for mutual understanding and engagement; to demonstrate a bit of flexibility in recognising alternative and equally respectable moral codes that were not established in ancient and very different times. But no.
Their recent performances on both voluntary assisted dying and marriage equality law reform suggest otherwise.
The fact is that to rebuild their franchises, the churches need to reach out to their Occasionals and to their Notionals — those who identify with the denomination but rarely if ever attend services. But the bishops have been pleasing only (some of) their Regulars and Devouts. It's a classic and literal case of “preaching to the converted.”
Voluntary assisted dying
In the matter of voluntary assisted dying (VAD) law reform, there are presently VAD Bills before both the NSW and Victorian parliaments. Figure 3 shows Australian attitudes toward VAD by religious affiliation.
Figure 3: Australian religious affiliation and attitudes toward VAD Source: AES 2016
Opposition to VAD amongst most denominations is very small, and really only makes an appearance amongst minor Christian and non-Christian denominations. Just 10% of Catholics and 7% of Anglicans oppose VAD, 5% and 3% of them strongly.
Figure 4 shows the real story. Opposition to VAD amongst Rejecters, Socialisers, Notionals and Occasionals is almost non-existent, and support is in a huge majority (85% of Socialisers, 89% of Notionals and 78% of Occasionals). Opposition to VAD amongst religion Rejecters is less than 2%. That is, opposition to VAD is almost entirely religious, although religious opposers pretend their opposition is nothing to do with faith.
Figure 4: Australian religious identity (ARI-6) and attitudes toward VAD Source: AES 2016
Only amongst Regulars and Devouts does opposition to VAD make a real appearance. Yet even amongst Devouts, with the strongest opposition, it’s in the minority (47%).
And what have the bishops been doing? They’ve campaigned strongly against VAD, spreading misinformation. Take for example the Catholic Church’s latest version of its anti-euthanasia polemic ‘brochure’ (Figure 5).
Figure 5: The Catholic Church’s latest polemic brochure against VAD Source: Catholic diocese of Byron Bay
This amateur production reveals a superficial understanding of the issues and a penchant for hyperbole. Worse, it employs significant misinformation in order to create FUD (fear, uncertainty and doubt), as does an advertisement taken out by a number of bishops from various denominations, in Melbourne’s major daily newspaper (Figure 6).
Figure 6: The June 2017 bishops' anti-VAD print advertisement Source: Herald Sun
The bishops’ manoeuvres will only alienate their congregation’s least committed members, the Notionals and Occasionals — the very people they should be wooing back to the pews, and who are strongly supportive of VAD as a valid and respectable response to intolerable and unrelievable suffering at end of life.
Perhaps the bishops would find this suggestion unpalatable, too much like a sales pitch. If that’s the case, one can only point out that selling the claim of saving of souls is the very task of evangelism. One could ask, “is your God likely to approve heartily of the continued withering of Australian faith?”
Marriage equality
The second contemporary example is marriage equality (ME). Figure 7 shows Australian attitudes to ME by religious denomination.
Figure 7: Australian religious affiliation and attitudes toward ME Source: AES 2016. Note: There was no ‘neither/nor’ option in this survey question
A clear majority of Australians in all groups except minor Christian denominations support marriage equality. That includes 74% of Catholics, 63% of Anglicans and 60% of Uniting Church members.
Figure 8 shows attitudes toward marriage equality by religious identity.
Figure 8: Australian religious identity (ARI-6) and attitudes toward ME Source: AES 2016
Support of marriage equality is in a clear majority amongst Rejecters (88%), Socialisers (82%), Notionals (73%) and Occasionals (71%). Around half (49%) of Regulars also support marriage equality.
Only amongst Devouts is support for marriage equality in the minority, with a quarter (25%) supporting and three quarters (75%) opposing it.
And what have the bishops been doing? They’ve run a massive campaign against marriage equality law reform. Indeed, the Anglican Archbishop of Sydney, Glenn Davies, announced that the diocese had donated, from precious church funds, $1 million to the ‘No’ campaign.
The public was even more dismayed to discover the diocese had granted just $5,000 to dealing with entrenched domestic violence in its ranks, at the same time as allocating the $1 million to preventing the equal expression of love.1
Given that marriage equality is almost certain to be legalised in Australia either directly after this voter ‘poll’ or in the term of the next Parliament, that’s an extraordinary squandering of a vast charitable sum for no net result. Calls have been made for the diocese’s tax-exempt status to be reviewed.
The evidence is incontestable: opposition to VAD is almost completely religious, and opposition to ME is largely religious, despite protestations to the contrary.
Bishops’ conduct in relation to these reforms, which most Australians want, have been unhelpful by resisting Australia’s move into the 21st century — on the basis of ancient interpretations of scripture to which only a small minority of Australians subscribe.
The bishops' conduct has run strongly counter to the compassion and understanding they could have shown in order to engage the Notionals and Occasionals amongst their flocks; to halt the erosion of their religious capital, and to rebuild it.
These bishops most certainly don't represent the general views and beliefs of most Australians on VAD or ME. Rather, they give the appearance of administrators who are determined to preside over smaller and smaller congregations: a kind of “slow euthanasia.”
To add insult to injury, it flip-flops on its stance.
Never mind that the argument is contradicted by evidence
The Church’s favourite argument — already contradicted by scholarly analysis that curiously seems to be of no interest to the Church — is this: if people are given the choice of assisted dying, they will feel compelled to choose it, coerced by doctors, greedy relatives or others; subtly or otherwise.
No matter that health care workers routinely report that relatives usually try and persuade their dying loved one to endure yet another invasive and burdensome treatment; not dissuade them from it.
The flip-flop
If the Catholic Church were indeed genuinely concerned about coercion of ‘the vulnerable,’ then it would equally oppose the right to refuse medical treatment, particularly if the treatment were life-prolonging. But it doesn’t.
If granny might die as a result of refusing a particular medical intervention, then a doctor might persuade her to refuse in order to conserve medical resources. Or greedy relatives might persuade her so that they are relieved of the burden and expense of looking after her and gain earlier access to her estate.
As eminent legal scholar Gerald Dworkin has argued,1 if there’s a theoretical ‘slippery slope’ for assisted dying, it’s the same for the refusal of life-preserving medical treatment.
To hold different positions under the same risks is to flip-flop. That’s especially so when there are numerous safeguards built into assisted dying statutes, but currently few or none for the right to refuse life-preserving medical treatment.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
Local experience confirms risk is theoretical
In my home state of Victoria, where the right to refuse any unwanted medical treatment has been enshrined in statute for nearly three decades (the Medical Treatment Act 1988), how many prosecutions have there been under the Act’s provisions against inappropriate persuasion?
Precisely none. Not a single case. So much for the theory.
It all serves to highlight that the Catholic Church’s only real argument is that it believes that it’s morally wrong to deliberately hasten death. However, it avoids this argument because as a religious tenet, it doesn’t appeal to the masses.
Catholic directives
The Church’s flip-flop about ‘the vulnerable’ is not a one-off accident. Take for example the ‘Ethical and Religious Directives for Catholic Health Care Services’ published by the United States Conference of Catholic Bishops.2
The Bishops ‘direct’ that there is no obligation on patients to use disproportionate means of preserving life. They state that disproportionate means are:
“…those that in the patient’s judgement do not offer a reasonable hope of benefit or entail an excessive burden, or impose excessive expense on the family or the community.”
The Bishops further ‘direct’ that:
“The free and informed judgment made by a competent adult patient concerning the use or withdrawal of life-sustaining procedures should always be respected and normally complied with, unless it is contrary to Catholic moral teaching.”
Setting aside the Church’s hubris of dishonouring the patient’s choice if the Church disagrees, it would be theoretically easy for someone to persuade the patient that hope was not reasonable, that the burden would be too great, or that the cost to the family or society would be too high.
Suffering for our God’s (your own) good
On the next page, the Bishops expressly ‘direct’ that:
“Patients experiencing suffering that cannot be alleviated should be helped to appreciate the Christian understanding of redemptive suffering.”
That’s unqualified. So, if you’re atheist, agnostic, Jewish, Hindu, Muslim or even a Christian who believes assisted dying can be appropriate, as a patient in their institutions you are to be persuaded that suffering against your beliefs and wishes is ‘redemptive’ in the eyes of the Vatican’s version of a God.
In Australia in 2009, for the Office for Family and Life in the Catholic archdiocese of Adelaide, Mr Paul Russell argued in News Weekly that “there is a point to suffering” because:
“It’s about the profound connection that each and every life has to the incarnate God … We know that the sufferings we endure well are joined in some mysterious way to the sufferings of Christ.”
Pity any poor soul who doesn’t share Mr Russell’s views. Curiously, there is no mention of this underpinning belief in his anti-assisted dying blog, “HOPE.”
Invalid argument in any case
The Church’s argument that ‘the vulnerable’ will be ‘at risk’ from assisted dying laws — for example in the Victorian Bishops’ recent pastoral letter to the Catholics of Victoria opposing the upcoming assisted dying parliamentary Bill — is itself fundamentally invalid.
That’s because, as I’ve previously explained, it’s a circular argument: a logical fallacy.
A circular argument: We must ban yellow socks on Wednesdays or the 'vulnerable' will be 'at risk'.‘The vulnerable,’ by definition are those ‘at risk,’ and will still be so if we wear yellow socks on Wednesdays. Therefore, we should ban such bright footwear midweek — and anything else we happen to oppose — on the same basis.
Might anyone suggest that “we should ban religion because the vulnerable will be at risk of succumbing to extreme religious views”?
Will the Church change its mind?
The Catholic Church does change its mind from time to time, though its reforms are glacially slow.
Take, for example, its theory of limbo, a place on the doorstep of hell where, the Church claimed, babies go if they die before they’re baptised: that they’d be prevented from entering heaven. It would be hard to imagine a crueller worry to put into the heads of uneducated new parents.
But in 2007, after centuries of confidently promoting the theory, the Catholic Church decided that it was wrong and buried it.
Will it change its mind on assisted dying? Maybe, but don’t hold your breath.
Conclusion
The Catholic Church, reeling from its extensive failure to protect our most vulnerable — children — and notwithstanding some good individuals within, still presumes to morally lecture the rest of us with the logical fallacy of how ‘risky’ assisted dying legislation is supposed to be to ‘the vulnerable,’ while flip-flopping in support of refusing life-saving medical treatment under the same theoretical risk.
The Bishops’ rhetoric amply exposes their confected crisis against assisted dying as nothing but religious doctrine draped in faux secular garb… in reality a sheep in wolves’ clothing.
References
Dworkin, G, Frey, RG & Bok, S 1998, Euthanasia and physician-assisted suicide, Cambridge University Press, Cambridge, New York. pp.66ff
Blog by Neil FrancisPosted on Saturday 24th September 2016 at 11:31pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
Against current moves to legalise assisted dying, Australian Catholic Father John George invokes Nazi Germany, resorts to ad hominem attacks to dismiss those who disagree with him, and demands that the Pope’s edicts are binding on everyone regardless of their own faith or world view.
On 24th September 2016, Journalists Greg Brown and Rick Morton published an article in The Australian, Victorian coroner credited with turning tide on euthanasia, summarising recent Australian moves to legalise assisted dying choice.
Catholic Father John George commented on the article online, quoting four sections of the Catholic Church’s catechism that prohibit assisted dying (sections 2276–9).
Pushback
Other readers of The Australian remarked that they respected his view for himself but they had no interest in the Pope’s views given the readers were not Catholic. In fact, repeated polls in Australia have shown that even the great majority of Catholics (three out of four) do not agree with the Vatican on the matter of assisted dying, a matter which Fr George dismisses merely as ‘fickle votes and polls.’
I would remind Fr George that these are not fickle: Australian public opinion in favour of assisted dying choice has been consistently in the majority for now more than four decades.
Fr George further quoted Catholic sources, for example the LJ Goody Bioethics Centre in Perth, Australia, which he failed to mention is, literally, an agency of the Catholic Archdiocese of Perth. He also selectively quoted Palliative Care Australia, failing to mention that they have acknowledged that not all pain and suffering can be eliminated at the end of life, even with the best palliative care.
Ad hominem attack
In response to a rising tide of objections to his musings, including from Mr Ian Wood, a fellow Christian and co-founder of Christians for Voluntary Euthanasia Choice, Fr George resorted to the ad hominem attack: to attack the person (or persons) rather than the arguments. He said:
“The pro euthanasia claque here make professional Nazi propaganda expert Goebbels look like a 5th rate amateur.” — Father John George.
For anyone in the dark, a claque is a group of sycophants hired to applaud a performer or public speaker. How rude. Fr George seems to have neglected to reflect that it is he who is hired to promote the performance of the Vatican. I applaud his right to do so, and I do not compare him to a treacherous propagandist in a murderous wartime regime in order to dismiss his arguments: I address the arguments themselves.
Nazi Germany
Fr George makes repeated mentions of Nazi Germany as a core reason to deny assisted dying choice.
In contrast, several years ago I was chatting at a conference with the pleasant and engaging Peter McArdle, then Research Director of the Australian Catholic Bishop’s Conference. He volunteered that he very much disliked the “Nazi Germany” argument so often used in religious circles, and wished it would stop because in so doing it meant they’d already lost the debate.
I agree. It’s a lazy and indefensible argument: that rational people in a functioning democracy must be denied choice for themselves on the basis of what some murderous regime did against others at the point of a gun.
Indeed, to rely on such a standard would be to equally argue against the right to religious practice, because the Catholic Church, through its inquisition practices (medieval C12th, papal C13th, Spanish C15th, Roman and Portuguese C16th) relied on torture and resulted in confiscation of property and at least tens (if not hundreds) of thousands of executions for witchcraft and heresy.
Ultimate hubris
But the real crux is that Fr George then unequivocally demands that:
“Principles elaborated by the pope are universally applicable.” — Father John George.
This ultimate hubris reveals a profound lack of self-reflection, both personally and organisationally. Even entertaining for a moment the premise that one individual (or even organisation) can tell everyone on the planet how they must live their lives, how would we choose that person or organisation? Why is it less valid for the head of any other branch of Christianity, of Judaism, Islam, Hinduism, Buddhism (or any other religion) or an agnostic (which I am) or an atheist, to set such rules for everyone, overriding other deeply-held beliefs and values?
A keener example of ‘blinded by faith’ would be hard to find.
Conclusion
I argue that Fr John George displays some of the gravest hubris of some members of the Catholic church. I respect and applaud his world views for himself and those who wish to subscribe. But using canonincal arguments (that is, religious arguments demanded as universally true by virtue of the supposed authority that dispensed them) is probably a major contributor to the current flight of people away from organised religion.
More happily, such an attitude is also contributing to accelerating the legalisation of assisted dying choice because folks can see these arguments for what they are. For that I doff my hat to Fr George.
Blog by Neil FrancisPosted on Saturday 3rd September 2016 at 4:44am
Mr Steve Jalsevac of the Catholic LifeSiteNews blog who made a shocking and vile attack.
I recently exposed (another) piece of misinformation published by LifeSiteNews, and wrote courteously to them to request withdrawal of the offending article. While I wasn’t hopeful the request would be accepted, I wasn’t prepared for the shocking and vile response I received.
Exposing bull about assisted dying is a key purpose of DyingForChoice.com and it will continue to do so as long as bull is published or publicly spoken, and especially when it makes claims or generates innuendo that is at odds with the readily-available facts, as a smokescreen for fundamentally religious objections.
The specific request to withdraw
In a recent article I factually rebutted the allegation by Mr Brad Mattes that there is suicide contagion (from assisted dying to general suicide) in Belgium, in addition to other statements that were wrong in fact in his opinion piece published by LifeSiteNews. I wrote a courteous letter to the editor of LifeSiteNews to point out the errors and to seek withdrawal of the article.
My full email to LifeSiteNews
Dear LifeSiteNews,
Clearly we are on different sides of the assisted dying conversation. I’m sure that we can mutually appreciate that different people bring different perspectives and apply some largesse in terms of world views.
However, one must draw the line (as your primary Principle does and upon which I think we agree) at the publication of information, however accidental, on your website that is in places fundamentally misleading and elsewhere quite false.
In this regard may I request that you withdraw the article by Mr Brad Mattes, Assisted suicide no longer just for the terminally ill, that contains multiple errors of evidential fact as well as fundamentally misleading statements, as I point out in this post?
Kind regards
Neil Francis
The shocking response
A firm believer in courteous debate even when one disagrees profoundly on important matters, I thought the most likely outcome would be a polite letter declining my request. But I received instead this response from LifeSiteNews Managing Director, Mr Steve Jalsevac.
Full response by Mr Steve Jalsevac of LifeSiteNews
Dear Neil,
I find it somewhat amusing that an advocate for legislation to allow people to kill themselves is demanding that we withdraw an article for supposedly publishing "misleading" or "false" information.
After many years of covering organizations such as yours which, typically cruelly manipulate vulnerable persons, violate or liberally interpret laws, understate their longer term objectives, have an extremely unhealthy and dangerous satisfaction in personally seeing people die before their eyes before their natural time, devastate family members whose loved ones had, unknown to them, been guided to kill themselves, and who have such perverse and wrong views on Christian beliefs and much more, I find it despicable that you would be so concerned about supposed accuracy. You, sir, are a hypocrite of the very worst kind.
It is our view that you should be behind bars for what you advocate and for your dangerous manipulation of vulnerable persons.
I realize that you will not agree with anything that I write given how blinded your conscience and intellect have become by your death preoccupation. So, I just conclude that your claims, views and interpretations are all rejected because no one should trust anything that you say or do on this subject.
Steve Jalsevac
LifeSite
Who is LifeSiteNews, anyway?
LifeSiteNews is an online blog established by the conservative Christian Campaign for Life Coalition. It promotes that it “emphasizes the social worth of traditional Judeo-Christian principles.” Its principles are all very courteously worded and sound “respectful” (its principles expressly use that word several times) whilst indicating that it is a pro-life blog.
I’ve read its articles on assisted dying for several years and have not found a single one that is at odds with the position of the Vatican. That’s hardly surprising.
LifeSiteNews publishes a significant proportion of articles about the Catholic Church, as is its right. It is also the sole publisher of Faithful Insight, in its own words “hard-hitting,” “100% faithful” and “fearless Catholic news coverage from the Vatican and beyond.” I argue strongly for the right to publish material of faith. That is not a source of complaint. (Fair disclosure—I’m agnostic.)
LifeSiteNews' hard-hitting and 100% Catholic-faithful publication.
And, Mr Jalsevac gives a clear indication that he’s at the 'Old School' end of the Catholic spectrum. He admires in multiple blogs the writings of conservative African Catholic Bishop Robert Sarah, noting John Paul II’s teachings as “definitive” and expressing disappointment in the current Pope. And that's entirely his right I again affirm.
Mr Jalsevac’s editor-in-chief, Mr John-Henry Westen has also published a number of articles critical of Pope Francis, also referring to previous Popes as more authoritative.
What do they claimto stand for?
LifeSiteNews’ first principle, in full, is this:
“1. Accuracy in content is given high priority. News and information tips from readers are encouraged and validated. Valid corrections are always welcome. Writing and research is of a professional calibre.”—LifeSiteNews.com
Mr Jalsevac's response highlights these claimed principles in stark relief by comprehensively breaching them.
The statements Mr Jalsevac makes about me are vile. And false. While I’m calling out his blogs’ misinformation for what it is, he’s calling for me personally to be thrown in jail for sins he falsely thinks I’ve committed. That’s squarely known as the ad hominem attack: attacking the person rather than the argument. It conveniently provides him with the excuse to totally ignore solid evidence that contradicts his beliefs.
Interestingly, an article by LifeSiteNews Editor Mr Westen quotes Pope Francis as saying,
“We Catholics have some — and not some, many — who believe in the absolute truth and go ahead dirtying the other with calumny, with disinformation…”—Pope Francis.
Quite.
Conclusion
LifeSiteNews is an 'Old School' Catholic blog, and, I argue, has every right to be.
However, it has demonstrated by publishing multiple articles containing serious errors of fact as well as highly misleading statements, and by a gratuitous ad hominem attack on someone pointing this out, that it is not interested in evidence, reason or even civility as it claims. In my view it has unambiguously demonstrated itself to be a biased and unreliable Catholic source on matters of assisted dying.
I will continue to call out misinformation in LifeSiteNews when I see it.
The F filesPosted on Friday 11th March 2016 at 9:42pm
He was red in the face and the veins on his neck were standing out. He involuntarily spat as he shouted while furiously jabbing a scientific journal paper high into the air. “This paper proves that palliative sedation doesn’t hasten death!,” he bellowed from the audience.
The recipient of the Catholic priest’s[§] ire was Dr Rodney Syme, who had just delivered a paper at a Catholic bioethics conference in Melbourne, Australia.
The presentation didn't win over an already skeptical audience given that his address was to argue, by referring to the scientific literature, that palliative care can’t always help alleviate refractory end-of-life symptoms and that continuous deep sedation (CDS) may hasten a patient’s death.
By the end of the address the audience was bristling with hostility and our priest bolted to his feet to commence the attack.
I hadn’t seen the journal paper the priest was brandishing, so immediately after the conference I retrieved a copy and studied it.1 You can obtain your own copy here.
But first, a little background on the doctrine of double effect.
Doctrine of double effect
There has been ongoing debate—both scholarly and otherwise—about whether CDS (particularly the administration of higher doses of opioids) for dying patients may hasten their death. CDS may be administered where the dying patient is suffering from intolerable and otherwise unrelievable symptoms, for the purpose of relief from those symptoms through the cessation of consciousness, even if it might hasten the patient's death.
To some, this is an uncontroversial medical intervention supported by the doctrine of double effect. The doctrine is widely attributed to thirteenth century Catholic Saint Thomas Aquinas, though he probably developed it from ancient Roman principles.
The doctrine says that it is acceptable to take this kind of action if it is proportionate to the suffering of the patient, that there are no other
less problematic alternatives, and that the doctor's intention is to relieve the suffering and not to hasten the patient’s death.
Skeptics of the doctrine point out that it can’t be reliably determined what the doctor was actually intending when they administered CDS prior to death. They also identify that the notion that it’s OK for a doctor to kill their patient (hasten her death) as long as the doctor “doesn’t really mean to,” is ethically questionable.
So, on the one hand the doctrine of double effect is relied upon to defend doctor actions, and on the other, it is claimed that CDS doesn’t hasten death in any case.
That’s having your cake and eating it too. If CDS didn’t hasten death, doctors wouldn’t need the doctrine of double effect as a defense.
Poor methodology
Back to the brandished paper. Having read it, I don’t understand how this paper passed peer review, assuming it was indeed peer reviewed. It’s a fact of life that on occasion, even prestigious journals like Lancet and the Journal of the American Medical Association publish manuscripts that shouldn’t see the light of day. I argue that this article (from Annals of Oncology) is one of them.
The research suffers from multiple, serious methodological problems.
The research suffers from multiple, serious methodological problems. Sure, the researchers attempted to match test patients (who received CDS) with control patients (who didn’t receive CDS), by age, class, gender, reason for admission and for functional status. But there the good work ends.
Here are some of the serious methodological flaws in the study.
Primary measure invalid. The authors report that they measured patient survival time from admission to hospice until death from any cause. This alone invalidates the entire study. If you say you are measuring the effects of CDS, then you have to measure from the commencement of CDS, not from some other event that is not the substance of your test.
Insufficient inclusion control. There is so much variability amongst the test and control subjects that the possibility of sufficient sensitivity to detect differences is highly unlikely. For example, around half of patients (53%) were admitted for uncontrolled symptoms of many and varied kinds but were not imminently dying, while a large minority (41%) were imminently dying. There was a wide range of cancer types from slow to aggressive, and of metastatic sites. The sheer breadth of patient contexts gave rise to a survival standard deviation (68% of observed variance, 6 days) that was 50% larger than the mean survival period (4 days). Translating that into 95% confidence (two standard deviations), the variance was three times larger (12 days) than the mean (4 days). Put another way, at 95% confidence, patients survived from minus 8 days to plus 16 days (from admission, not administration of CDS). Hardly the stuff to drive assertive conclusions.
Insufficient intervention assessment. The researchers considered only the administration of sedatives, not of any other medical or palliative interventions in their assessment of patient survival. What other interventions were administered, when and in what amount, and how successful were they? The authors also assumed that any necessary nutrition and hydration was given to patients (whether natural or by tube) equally across hospice units because “the best palliative care should be provided.” There was no mention of whether the various units had identical (or any) written palliative care practice standards or whether those standards were known and actually practiced by attending physicians and nurses in patient cases for this study.
Insufficient intervention control. A wide range of sedative types (not just opioids) were administered in a wide range of doses for widely ranging periods of time; from sudden, light and intermittent, to heavy and continuous. Around half the patients receiving sedation received multiple different sedatives.
It is hardly surprising then, given this sorry state of affairs, that the study failed to find a significant difference in ‘survival’ between test and control groups: the design was certain to result in insufficient sensitivity. (Curiously, the CDS patients survived on average longer (12 days) than the control patients (9 days), though the difference was not statistically significant.)
Unscientific conclusion
In scientific studies—particularly those which have yet to be successfully replicated by other researchers—best practice dictates that the minimum ‘significance’ is cautiously attributed to the results. The minimum significance in this case would be that “our study did not find evidence to support the contention that administration of sedation hastens patient death”.
The conclusion asserted by the researchers
is not established by the study.
The next level of attribution is still cautious, but a little more assertive: “the results suggest that the administration of sedation doesn’t hasten patient death”. It is my belief, especially given the poor design and conduct of the study, that this level of attribution would be too high.
But the authors went all out. They categorically concluded that “PST [palliative sedation therapy] does not shorten life” and trumpeted it in the article’s title: “Palliative sedation therapy does not hasten death.” On the basis of this unjustifiable interpretation they further categorically concluded that the doctrine of double effect is therefore unnecessary.
The authors in my view committed a serious scientific blunder in translating an exploratory and poorly-designed study into unqualified and assertive, unsupported conclusions. How this passed peer and editorial review is a mystery.
The upshot
The upshot of this is that our priest, perhaps with an understandable deficit of expertise in scientific endeavour, grabbed a paper that supported his hypothesis and fervently believed it to provide unarguable evidence, given its unequivocal title and conclusion.
In reality, each and every paper published in scientific journals has to be read and judged on its own merits. It is not appropriate to simply accept a study’s conclusions merely by virtue of its publication in a journal, even a prestigious one.
In reality, each and every paper published in scientific journals has to be read and
judged on its own merits.
Critical appraisal (including cross-checking other sources) is the scientific standard of practice I employ as I follow trains of research and commentary on various facets of end-of-life decisions and assisted dying, across my literature collection now well in excess of five thousand journal articles, theses, books, professional policy papers and other sources.
It is a standard I commend to everyone in order to hone in on the truth and to avoid dissemination of flapdoodle, fudge and fiction.
References
1 Maltoni, M, Pittureri, C, Scarpi, E, Piccinini, L, Martini, F, Turci, P, Montanari, L, Nanni, O & Amadori, D 2009, 'Palliative sedation therapy does not hasten death: results from a prospective multicenter study', Ann Oncol, 20(7), pp. 1163-9.
[§] The meeting was conducted under Chatham House rules, so what was said can be reported, but who said it cannot.
Blog by Neil FrancisPosted on Wednesday 25th November 2015 at 8:00pm
St Patrick's Cathedral, Melbourne, Australia. Photo: Donaldytong
On Wednesday 19th November 2015, the Catholic Church appeared before the Victorian Parliament's Legal and Social Issues Committee. Monsignor Anthony Ireland, the Episcopal Vicar for Health, Aged and Disability Care, and Father Anthony Kerin, Episcopal Vicar for Life, Marriage and Family gave evidence about end-of-life decision making. They made a factually wrong allegation about Oregon during their testimony.
Anthony Ireland spoke first, making it clear that they were appearing before the Committee with delegated authority from the Catholic Archbishop of Melbourne (Denis Hart) and with the endorsement of the Victorian Catholic Bishops. He emphasised that "the Catholic Archdiocese of Melbourne does not come to this Committee with fanciful or frivolous arguments."
During question time. Committee Chair Edward O'Donohue asked the Vicars if they had any evidence from lawful jurisdictions to back up their claim that legalising assisted dying would result in a significant reduction in medical research. The Vicars flailed about with vague hypotheticals, but no evidence.
Committee Deputy Chair Nina Springle remarked that some of their testimony was inconsistent with direct evidence from lawful jurisdictions and invited them to reflect on the contradictions. To this, Anthony Kerin stated:
"We know, for example, since Oregon legislated, that the standard suicide rate has increased remarkably and alarmingly. It's not yet the largest rate in the US, but it's getting there, when Oregon had a very, very low suicide rate prior to that."
Let's not mince words: the allegation is comprehensively false. In fact it's three false statements all wrapped up into one.
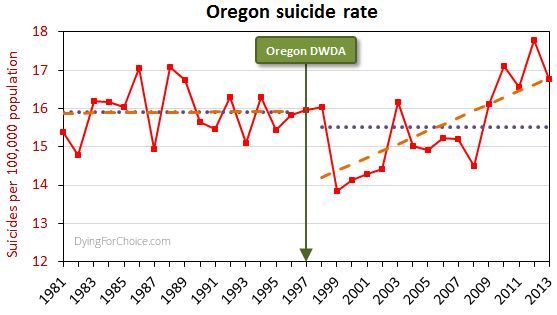
The USA government's CDC mortaility database provides solid empirical data. Here's Oregon's longitudinal suicide rate statistics, including sixteen years before its Death With Dignity Act (DWDA), and sixteen years after.
Here are the pertinent facts about Oregon's general suicide rate:
The average for the 16 years after the DWDA is lower than, but not statistically different from, the 16 years prior to the Act.
There was a massive drop in the suicide rate two years after the DWDA came into effect, and the rate has risen only from there.
The rise from 2000 onwards is repeated in the majority of USA states and in the national average. The trend increase in Oregon is not statistically different from the national trend increase.
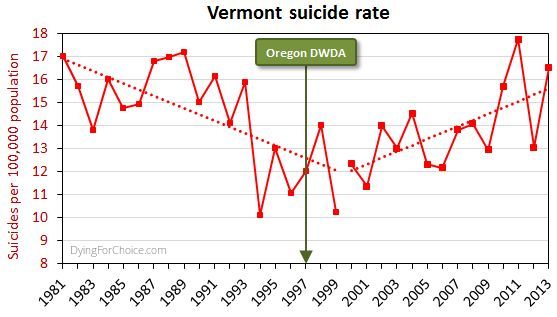
By way of comparison, here's Vermont's suicide rate for the same period.
Now, Vermont didn't have an assisted dying law until 2013, and no assisted deaths occurred under the law in that year, so the suicide rate cannot have been affected by an assisted dying law. Yet the picture is similar to Oregon's.
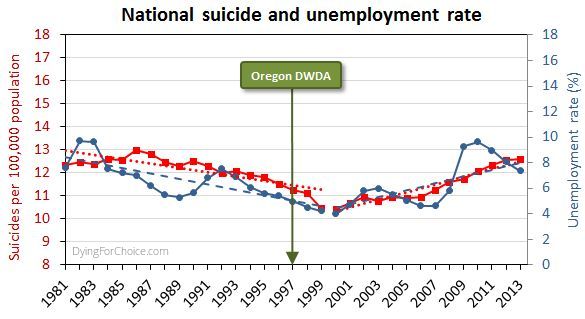
Here's the USA national suicide rate for the same period, with the unemployment rate added.
There are numerous and complex reasons for suicide and for changes in the rate, but a key one in this USA case is unemployment, which after falling in the 1990s rose abruptly from 2000 onwards.
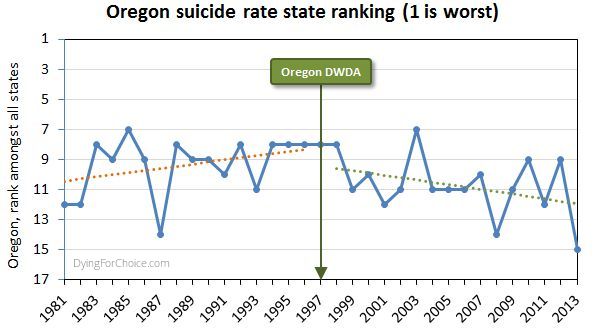
Has Oregon's suicide rate been worsening relative to other USA states, though? The state annual suicide rankings are informative.
Prior to the DWDA, the trend in Oregon's suicide ranking among all USA states was deteriorating (where ranking number one is the highest suicide rate). Since the Act came into effect, the trend is improving. The difference in trends is statistically significant. In the sixteen years since the Act came into effect, Oregon has appeared in the "top ten" six times, compared with twelve times in the 16 years prior to the Act.
So, let's examine the three elements of the Catholic Church's statement:
1. "Since Oregon legislated, the standard suicide rate has increased remarkably and alarmingly"
This statement is false by omission. It is critically relevant to mention that Oregon's suicide rate dropped massively two years after the DWDA came into effect. Only after 2000 did it begin to rise—like most states and nationally—and in response to a rising unemployment rate.
2. "Oregon had a very, very low suicide rate prior to that [the DWDA]"
This statement is completely false. Oregon's mean rate suicide for 16 years after the act is not significantly different from the mean for 16 years prior to the Act. Indeed, government data back to 1968 shows Oregon's general suicide rate has always been high and never "low", let alone "very, very low".
3. It's not yet the largest rate in the US, but it's getting there"
This statement is completely false. Oregon's suicide ranking amongst USA states was worsening prior to the DWDA, but has been improving since.
It's very disappointing indeed that the Catholic Archdiocese of Melbourne would offer such profoundly false testimony to a legislative committee making inquiries on behalf of the people of Victoria. The offense is all the more grevious because of the unequivocal manner in which the statement was made, and that the witnesses specifically stated they did not bring any fanciful or frivolous arguments to the Committee.
It's time to comprehensively stamp out false information about assisted dying, no matter how fervently it might be believed by its proponents. Watch this space: there's plenty more to come!
News reportPosted on Monday 5th October 2015 at 4:15pm
On Friday September 11th 2015, the California legislature passed an assisted dying bill, the End Of Life Option Act, modelled on the Oregon Death With Dignity Act which has been in effect since 1997. It had been a long and tortuous wait to see if Governor Jerry Brown would sign the Bill into law.
It is reported that Governor Brown struggled to decide whether to sign the Bill which was actively opposed by the Catholic Church. Governor Brown is a former Jesuit seminary student. He sought views from his doctors, from a Catholic Bishop, from disability advocates, retired South African Archbishop Desmond Tutu and others, to reach a decision. While he had given no indication of his views or intention to sign, historically he has supported abortion rights, contrary to the teachings of the Vatican.
On Monday October 5th, he signed the Bill. It will come into effect 90 days after the California legislature adjourns its special session on healthcare. But that may not be for some months yet, even as long as late next year.
Governor Brown said "I have considered the theological and religious perspectives that any deliberate shortening of one's life is sinful."
"I do not know what I would do if I were dying in prolonged and excrutiating pain. I am certain, however, that it would be a comfort to be able to consider the otpions afforded by this bill. And I wouldn't deny that right to others," he wrote in his affirmation of the Bill.
California joins Oregon, Washington, Montana and Vermont to afford their citizens the respect to make their own decicions about the possibility of a hastened death at the end of life. Around one in six Americans now has legal access to restricted assisted dying.
Dissatisfied that the legislature and the Governor have spoken on behalf of the overwhelming majority of Californians who support the measure, Catholic-backed Californians Against Assisted Suicide is considering a range of countermeasures, including a legal challenge and a referendum.
 The Kellogg's Sultana Bran TV commercial from 1990.
The Kellogg's Sultana Bran TV commercial from 1990.

 Figure 1: Australian religious affiliation by census year
Figure 1: Australian religious affiliation by census year") Figure 2: Australian denominations and Australian religious identity (ARI-6)
Figure 2: Australian denominations and Australian religious identity (ARI-6) Figure 3: Australian religious affiliation and attitudes toward VAD
Figure 3: Australian religious affiliation and attitudes toward VAD and attitudes toward voluntary assisted dying") Figure 4: Australian religious identity (ARI-6) and attitudes toward VAD
Figure 4: Australian religious identity (ARI-6) and attitudes toward VAD Figure 5: The Catholic Church’s latest polemic brochure against VAD
Figure 5: The Catholic Church’s latest polemic brochure against VAD Figure 6: The June 2017 bishops' anti-VAD print advertisement
Figure 6: The June 2017 bishops' anti-VAD print advertisement Figure 7: Australian religious affiliation and attitudes toward ME
Figure 7: Australian religious affiliation and attitudes toward ME Figure 8: Australian religious identity (ARI-6) and attitudes toward ME
Figure 8: Australian religious identity (ARI-6) and attitudes toward ME
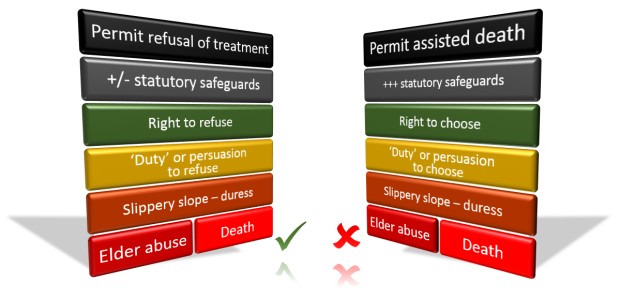 The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.