Blog by Neil FrancisPosted on Friday 1st February 2019 at 8:55pm
Colorado has just released its second annual assisted dying report
The USA state of Colorado legalised assisted dying via its End Of Life Options [#145] Act in 2016. Its Department of Public Health & Environment has just published its second annual report of statistics of medications dispensed and deaths.
Unfortunately, the Colorado statistics report only all deaths of those prescribed life-ending medications, not those who died using the medication.
In 2017, 70 people who had been prescribed life-ending medication died, representing 0.19% of all deaths.* With Oregon and Washington states clearly showing around 30% of people prescribed lethal medication die without using it, that represents 49 people and 0.13% of all deaths.
In 2018, 104 people who had been prescribed life-ending medications died, representing 0.28% of all deaths. Adjusted to those who would have used their medication, that represents 73 people and 0.20% of all deaths.
The 2017 data is very similar to California's, which also legalised assisted dying in 2016. In 2017, 0.15% of Californians died using its End Of Life Options Act, with 35% of those who had been prescribed the medication having not used it. (California's 2018 annual report has not been released yet.)
The End Of Life Options Acts of both states stipulate that to qualify, a person must be an adult with decision-making capacity and have a terminal illness with death anticipated within six months. Patients may self-administer lethal medication prescribed by their physician: no other person may administer.
-----
* Total deaths official statistics for Colorado and California not yet available for 2017/2018: total deaths for 2017 and 2018 were calculated using linear extrapolation of USA Centers for Disease Control total deaths data for 1999-2016.
The F filesPosted on Saturday 18th November 2017 at 11:27pm
Jones, Paton and Kheriaty's articles demonstrate poor science and multiple, egregious instances of bias.
In 2015, Dr David Jones and Prof. David Paton published an article titled “How does legalization of physician-assisted suicide affect rates of suicide?” in the Southern Medical Journal. The article purported to establish suicide contagion from Oregon and Washington Death With Dignity Act (DWDA) deaths to “total suicides.” It also purported to establish no decrease in general suicide rates, which Jones & Paton argued should occur by substitution of assisted death for some general suicides. (Notice how these two ‘expected’ results — an anticipated rise and an anticipated fall in suicide rates — are at odds in principle.)
In my thorough and empirically-backed response, I expose the disgraceful playbook of these authors as they shambolically commit no fewer than ten deadly sins against science in the pursuit of their opposition to lawful assisted dying.
In 2015, Dr David Jones & Prof. David Paton published an article in the Southern Medical Journal titled “How does legalization of physician-assisted suicide affect rates of suicide?” This study examines the article, as well as an enthusiastic editorial of it by Dr Aaron Kheriaty in the same journal issue, both of which portray “suicide contagion” from Oregon and Washington’s death with dignity acts (DWDA).
However, while contagion from general suicides is a well-established phenomenon, there are multiple sound reasons to reject contagion theory in relation to assisted deaths, including:
Most healthcare professionals readily acknowledge key differences in the characteristics of assisted deaths: for example, a fully informed, tested and rational decision with shared decision-making.
Those using Oregon and Washington’s DWDAs are, by qualifying for it, already actively dying. Thus, they are choosing between two ways of dying rather than between living and dying.
Most of those using the DWDA discuss it with their families (expected, peaceful death), whereas most general suicides occur in isolation and without discussion (unexpected, often violent death).
Multiple studies show that while families of general suicide experience complicated bereavement, families of assisted dying cope at least as well as, and in some cases better than, the general population or those who considered but did not pursue assisted death.
Even if “suicide contagion from assisted dying” theory were sound, direct evidence from official government sources shows that the number of potential suicides in Oregon in 2014 would have been fewer than 2 in 855 cases: undetectable by general modelling methods.
Jones & Paton’s article title conveys an air of skilled and scientific neutrality. However, close examination of the article, and Kheriaty’s editorialisation of it, reveals least ten serious flaws or ‘scientific sins.’
The authors demonstrated little understanding of the complex issues surrounding suicide, willingness to unjustifiably equate assisted dying with general suicide, contentment with failing to search for, consider or include contrary evidence including from sources they cite to argue their case, unreasonable trust in a model that couldn’t hope to legitimately resolve their premises, satisfaction with executing their model amateurishly, a disposition to overstate confidence of causation in the absence of meaningful statistical correlations, and an inclination for emphasising results in accordance with their theories while de-emphasising or ignoring others.
Any of these flaws was serious enough to invalidate Jones & Paton’s article and Kheriaty’s conclusions of it, yet there is not one deadly flaw: there are at least ten.
Their claim of a supposed 6.3% suicide contagion rate from assisted dying in Oregon and Washington is a conceptual and mathematical farce.
The Southern Medical Journal is a peer-reviewed journal. However, it is difficult to reconcile the rigorous standards and sound reputation that peer review is intended to maintain, with the numerous, egregious flaws in this study and its dissemination.
Rather than inform the ongoing conversation about lawful assisted dying, the Jones & Paton and Kheriaty articles misinform and inflame it.
Given the numerous egregious flaws, both articles ought to be retracted.
Blog by Neil FrancisPosted on Monday 13th November 2017 at 6:28pm
The deeply-flawed Jones & Paton, and Kheriaty articles purporting to show suicide contagion.
In the ongoing political campaign against assisted dying law reform, opponents have spread one piece of egregious misinformation after another. One of the most common is supposed “suicide contagion” from assisted dying laws to general suicide, a theory popularised by Catholic Prof. Margaret Somerville. Despite the nonsense of her claim being comprehensively exposed, she still believes that her opinion “will prove to be correct.” Two journal papers published in 2015 purported to, but didn't, establish suicide contagion in Oregon and Washington states.
Assisted dying law reform opponents are still relying on a 2015 paper by Catholics David Jones and David Paton, bolstered by a glowing editorial of it written by Catholic psychiatrist Aaron Kheriaty, published in the Southern Medical Journal, as continued ‘proof’ of suicide contagion theory, at least in respect of USA states Oregon and Washington (since data from other lawful jurisdictions contradicts the theory).
Jones & Paton’s article reported the use of econometric modelling to test for ‘suicide contagion’ from Oregon and Washington’s Death With Dignity Act (DWDA) laws. But, in an exposé to be published this week, no fewer than ten ‘deadly sins’ of the study are peeled back to reveal the rot within.
The very deep flaws and biases of the original articles include:
Cherry-picking information from cited sources to argue their case, while omitting information from the same sources that contradicted their case;
Including test and control subjects whose consequence was likely to maximise the likelihood of finding a positive association;
Demonstrating a poor understanding of suicide and its risk and protective factors and failing to control for most confounding effects in their econometric model ‘pudding’;
Overegging the “causative suicide contagion” interpretation when no correlation between assisted dying and general suicide rates was found; and
Failing to use direct, robust and readily-available evidence that showed their study couldn’t possibly have hoped to return scientifically valid “contagion” proof.
The USA’s National Violent Death Reporting System (NVDRS), of which Oregon is a founding member, shows that even if “assisted dying suicide contagion theory” were true, fewer than 2 of 855 Oregon “total suicides” in 2014 could have been attributed to “contagion” from DWDAs.
Further, both Oregon and Washington state rankings for suicide rates have improved, not deteriorated, since their DWDAs came into effect, while the suicide ranking for a relevant control state — Oklahoma — has deteriorated substantially over the same time.
Ultimately, through numerous and deep methodological flaws, the Jones, Paton and Kheriaty articles reveal a bias to promote “assisted dying suicide contagion theory” while ignoring the robust evidence from multiple lawful jurisdictions, including in their own ‘study,’ that contradict it.
The exposé, titled “The ten deadly sins of Jones, Paton and Kheriaty on ‘suicide contagion’,” will be published by DyingForChoice.com later in the week.
To add insult to injury, it flip-flops on its stance.
Never mind that the argument is contradicted by evidence
The Church’s favourite argument — already contradicted by scholarly analysis that curiously seems to be of no interest to the Church — is this: if people are given the choice of assisted dying, they will feel compelled to choose it, coerced by doctors, greedy relatives or others; subtly or otherwise.
No matter that health care workers routinely report that relatives usually try and persuade their dying loved one to endure yet another invasive and burdensome treatment; not dissuade them from it.
The flip-flop
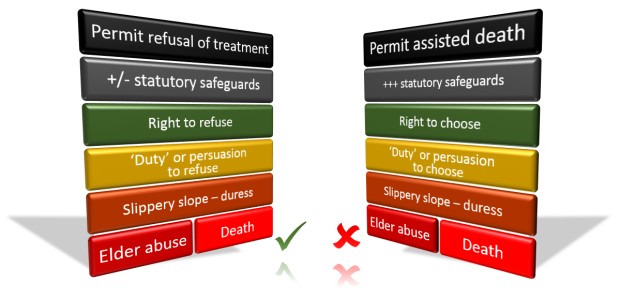
If the Catholic Church were indeed genuinely concerned about coercion of ‘the vulnerable,’ then it would equally oppose the right to refuse medical treatment, particularly if the treatment were life-prolonging. But it doesn’t.
If granny might die as a result of refusing a particular medical intervention, then a doctor might persuade her to refuse in order to conserve medical resources. Or greedy relatives might persuade her so that they are relieved of the burden and expense of looking after her and gain earlier access to her estate.
As eminent legal scholar Gerald Dworkin has argued,1 if there’s a theoretical ‘slippery slope’ for assisted dying, it’s the same for the refusal of life-preserving medical treatment.
To hold different positions under the same risks is to flip-flop. That’s especially so when there are numerous safeguards built into assisted dying statutes, but currently few or none for the right to refuse life-preserving medical treatment.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
Local experience confirms risk is theoretical
In my home state of Victoria, where the right to refuse any unwanted medical treatment has been enshrined in statute for nearly three decades (the Medical Treatment Act 1988), how many prosecutions have there been under the Act’s provisions against inappropriate persuasion?
Precisely none. Not a single case. So much for the theory.
It all serves to highlight that the Catholic Church’s only real argument is that it believes that it’s morally wrong to deliberately hasten death. However, it avoids this argument because as a religious tenet, it doesn’t appeal to the masses.
Catholic directives
The Church’s flip-flop about ‘the vulnerable’ is not a one-off accident. Take for example the ‘Ethical and Religious Directives for Catholic Health Care Services’ published by the United States Conference of Catholic Bishops.2
The Bishops ‘direct’ that there is no obligation on patients to use disproportionate means of preserving life. They state that disproportionate means are:
“…those that in the patient’s judgement do not offer a reasonable hope of benefit or entail an excessive burden, or impose excessive expense on the family or the community.”
The Bishops further ‘direct’ that:
“The free and informed judgment made by a competent adult patient concerning the use or withdrawal of life-sustaining procedures should always be respected and normally complied with, unless it is contrary to Catholic moral teaching.”
Setting aside the Church’s hubris of dishonouring the patient’s choice if the Church disagrees, it would be theoretically easy for someone to persuade the patient that hope was not reasonable, that the burden would be too great, or that the cost to the family or society would be too high.
Suffering for our God’s (your own) good
On the next page, the Bishops expressly ‘direct’ that:
“Patients experiencing suffering that cannot be alleviated should be helped to appreciate the Christian understanding of redemptive suffering.”
That’s unqualified. So, if you’re atheist, agnostic, Jewish, Hindu, Muslim or even a Christian who believes assisted dying can be appropriate, as a patient in their institutions you are to be persuaded that suffering against your beliefs and wishes is ‘redemptive’ in the eyes of the Vatican’s version of a God.
In Australia in 2009, for the Office for Family and Life in the Catholic archdiocese of Adelaide, Mr Paul Russell argued in News Weekly that “there is a point to suffering” because:
“It’s about the profound connection that each and every life has to the incarnate God … We know that the sufferings we endure well are joined in some mysterious way to the sufferings of Christ.”
Pity any poor soul who doesn’t share Mr Russell’s views. Curiously, there is no mention of this underpinning belief in his anti-assisted dying blog, “HOPE.”
Invalid argument in any case
The Church’s argument that ‘the vulnerable’ will be ‘at risk’ from assisted dying laws — for example in the Victorian Bishops’ recent pastoral letter to the Catholics of Victoria opposing the upcoming assisted dying parliamentary Bill — is itself fundamentally invalid.
That’s because, as I’ve previously explained, it’s a circular argument: a logical fallacy.
A circular argument: We must ban yellow socks on Wednesdays or the 'vulnerable' will be 'at risk'.‘The vulnerable,’ by definition are those ‘at risk,’ and will still be so if we wear yellow socks on Wednesdays. Therefore, we should ban such bright footwear midweek — and anything else we happen to oppose — on the same basis.
Might anyone suggest that “we should ban religion because the vulnerable will be at risk of succumbing to extreme religious views”?
Will the Church change its mind?
The Catholic Church does change its mind from time to time, though its reforms are glacially slow.
Take, for example, its theory of limbo, a place on the doorstep of hell where, the Church claimed, babies go if they die before they’re baptised: that they’d be prevented from entering heaven. It would be hard to imagine a crueller worry to put into the heads of uneducated new parents.
But in 2007, after centuries of confidently promoting the theory, the Catholic Church decided that it was wrong and buried it.
Will it change its mind on assisted dying? Maybe, but don’t hold your breath.
Conclusion
The Catholic Church, reeling from its extensive failure to protect our most vulnerable — children — and notwithstanding some good individuals within, still presumes to morally lecture the rest of us with the logical fallacy of how ‘risky’ assisted dying legislation is supposed to be to ‘the vulnerable,’ while flip-flopping in support of refusing life-saving medical treatment under the same theoretical risk.
The Bishops’ rhetoric amply exposes their confected crisis against assisted dying as nothing but religious doctrine draped in faux secular garb… in reality a sheep in wolves’ clothing.
References
Dworkin, G, Frey, RG & Bok, S 1998, Euthanasia and physician-assisted suicide, Cambridge University Press, Cambridge, New York. pp.66ff
Blog by Neil FrancisPosted on Sunday 19th March 2017 at 11:37pm
Oregon (left) and Washington legalised assisted dying by ballot in 1997 and 2008 respectively. Photos: Oregon Department of Transportation; Cacophony.
A scientific study just published in the New England Journal of Medicine reveals that residents of both Oregon and Washington states, which legalised assisted dying in 1997 and 2008 respectively—as well as establishing formal advance directive programs—are far more likely to experience the kind of death they prefer, and with better access to palliative care, than is the average USA resident.1
It's well-established that most westerners would prefer to die peacefully at home rather than in a medicalised or other institutional setting. Yet it is recognised by doctors and families alike that there is a kind of medical ‘conveyer belt’ to acute care at the end of life that tends to shunt the dying individual through to ICU—a place where more and more burdensome medical interventions are administered with less and less likelihood that they’ll actually provide any benefit. These kinds of deaths, with vigorous and invasive procedures performed on a frail person approaching a natural death, can lead to longer and more complex bereavement recovery for surviving loved ones.
It’s also claimed by opponents of assisted dying law reform that assisted dying is a ‘competitor’ of palliative and hospice care, and that legalisation of assisted dying would result in the deterioration or at least stunting of palliative care services.
This latest study, including longitudinal data, provides further evidence that such claims are not only false, but that the legalisation of assisted dying improves the focus on all end of life decision making, whatever those decisions are.
Avoiding burdensome and questionable invasive care
Figure 1: ICU was used in the last 30 days of life Percent of fee-for-service Medicare service beneficiary patients
Figure 1 shows that the ‘shunting’ of dying patients to ICU in the last 30 days of life is significantly lower in Oregon, which legalised assisted dying in 1997. Oregon also established a statutory comprehensive advance care directive (Physician Orders for Life Sustaining Treatment, or “POLST”) program earlier than other states, in 1993. Washington, which piloted a POLST program in 2000 and formally endorsed it in 2005 — and legalised assisted dying by ballot in 2008 — was already trending down from the national average (close to it in 2000), as public discussion of end of life decisions ratcheted up in the lead-up to reform. Since the POLST endorsement and ballot reform, Washington has continued to trend well below the national average.
Facilitating a non-institutionalised death
Figure 2: Patient was discharged from hospital in the last 30 days of life
Figure 2 shows that both Oregon and Washington have continued to trend above the national average for facilitating patient wishes to die at home after a stay in acute care in the last 30 days of life.
Hospice care received at home
Figure 3: Dying patient received hospice care at home
Figure 3 shows that by 2000, Oregon was already providing home hospice services at 2.1 times the national average, but that as the national average plateaued from 2005, the rate in Oregon continued to rise significantly, reaching 2.5 times the national average in 2013. To qualify for an assisted death, Oregon and Washington residents must be certifed by their doctor as expected to die within six months—which qualifies the patient for free hospice care.
Washington was close to the national average on the delivery of home hospice care prior to assisted dying law reform, beginning to deviate as conversations were held about permitting assisted dying and its POLST program was endorsed in 2005, increasing to 1.8 times the national average in 2013.
Death preferred at home
Figure 4: The individual died at home
Figure 4 shows that both Oregon and Washington states continue to facilitate a private home-based death, according to patient and family wishes, at a rate considerably higher than the national average.
Conclusion
The results of this USA study mirror the kinds of findings from Dutch and Belgian research, which I have previously published,2 and another USA report from the Journal of Palliative Medicine which placed both Oregon and Washington amongst the top eight states for palliative care access in hospital settings.3 This study furthers these insights by showing that access to palliative care services in home settings is also significantly higher than the national average in Oregon and Washington.
Assisted dying opponents’ claims that legalising assisted dying would result in a deterioration or stunting of end of life decisions and in particular access to palliative care are contradicted by the data from lawful jurisdictions.
References
Tolle, SW & Teno, JM 2017, 'Lessons from Oregon in embracing complexity in end-of-life care', New England Journal of Medicine, 376(11), pp. 1078-1082.
Morrison, RS, Augustin, R, Souvanna, P & Meier, DE 2011, 'America's care of serious illness: A State-by-State report card on access to palliative care in our nation's hospitals', Journal of Palliative Medicine, 14(10), pp. 1094-1096.
Blog by Neil FrancisPosted on Sunday 5th March 2017 at 10:24pm
Alex Schadenberg's latest shrill and misleading article
Catholic Canadian anti-assisted-dying blogger Alex Schadenberg is at it again. This time he’s parading his ignorance and spreading bull about a potential change in Oregon’s assisted dying legislation.
The Bill
Mr Schadenberg correctly reproduced Section 3 of Oregon Senate Bill 893, which states:
SECTION 3. An expressly identified agent may collect medications dispensed under ORS 127.815 (1)(L)(B)(ii) and administer the medications to the patient in the manner prescribed by the attending physician if:
(1) The patient lawfully executed an advance directive in the manner provided by ORS127.505 to 127.660;
(2) The patient’s advance directive designates the expressly identified agent as the person who is authorized to perform the actions described in this section;
(3) The patient’s advance directive includes an instruction that, if the patient ceases to be capable after medication has been prescribed pursuant to ORS 127.800 to 127.897, the expressly identified agent is authorized to collect and to administer to the patient the prescribed medication;
(4) The medication was prescribed pursuant to ORS 127.800 to 127.897; and
(5) The patient ceases to be capable.
Mr Schadenberg fails to mention Section 2, which states:
SECTION 2. Section 3 of this 2017 Act is added to and made a part of ORS 127.800 to 127.897.
What is the ORS range?
And what precisely is ‘ORS 127.800 to 127.897’ (ORS = Oregon Revised Statutes)? Why, it’s the entirety of Oregon’s existing Death With Dignity Act!
In other words, a patient still has to be terminally ill, fully informed, made a formal request, the request assessed as genuine and free, waited the required cooling off period, made another formal request, been assessed as qualifying all the requirements by multiple doctors, has legally appointed an agent expressly for the purpose of administering lethal medication pursuant to the Death With Dignity Act, have their medication prescribed (immediately before which the attending physician must again verify that the patient is making an informed decision) and then the patient ceases to be capable, before the agent may then administer.
Mr Schadenberg exposes that at best he fundamentally doesn’t understand the Bill, nor took much if any effort to do so.
That’s hardly the free-for-all Mr Schadenberg posits in his shrill blog implying that ‘assisted suicide and euthanasia’ was being extended to ‘incompetent people’ without further qualification; falsely insinuating that any incompetent person could then obtain assistance for suicide or euthanasia.
No ‘defence’
If Mr Schadenberg were to claim that he really meant ‘only within the scope of the current Death With Dignity Act,’ and that he’s been taken out of context, that simply won’t wash. Bill 893 makes a provision only for someone else to administer the lethal dose (that is, what Mr Schadenberg refers to as ‘euthanasia’) if the patient ceases to be capable after already qualifying under the existing Act. The Bill does not permit patient self-administration: that is, using Mr Schadenberg’s own language, ‘assisted suicide’—which he expressly refers to in his article.
Parading a non-existent extension of ‘assisted suicide’ clearly exposes that at best he fundamentally doesn’t understand the Bill, nor took much if any effort to do so.
Wrong again…
He also got it completely wrong as to who may administer when the patient ceases to be capable:
“The bill enables the doctor to administer…” — Alex Schadenberg
However, if you read Section 3 of the Bill (above) that Mr Schadenberg himself reproduces, you’ll see clearly that the patient must expressly identify a particular person ('agent') to administer lethal medication should the patient cease to be capable. The patient may appoint his or her doctor, but can appoint in their Advance Care Directive anyone to be the agent; including a trusted and loved family member. The only particular requirement for the agent’s administration is that he or she must “administer in the manner prescribed by the attending physician.”
Conclusion
But let’s not the facts get in the way of a gratuitous reaction trumpeting shrill hyperbole and headline, shall we Mr Schadenberg?
And as usual, Catholic Australian anti-assisted-dying blogger Paul Russel has dutifully reproduced Mr Schadenberg’s farce.
“#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
Her just-published IAHPC ‘Concept Note’ railing against assisted dying,1 and summarised on the European Association of Palliative Care’s (EAPC) website,2confirms and amplifies precisely the point I made.
Now you’d think that an organisation with a name like ‘International Association for Hospice and Palliative Care’ would be a neutral organisation representing the world profession irrespective of the faith or personal spiritual beliefs of its members.
But you’d be quite wrong.
Nothing but Catholic doctrine
The IAHPC's musings extensively cite several Popes as the authorities on the subject of — and exclusively against — assisted dying. They expressly use the term "Table of authorities," which includes Popes. And who else?
Precisely nobody: no other faith, and no impartial scientific research, is cited. Just Popes.
She also writes:
“IAHPC wishes to encourage our partners to express clear support for faith based teachings on palliative care.”
“It is important to clarify this misinformation [about ‘stealth euthanasia’] with the authoritative teachings of the Church.”
“Hospice has always been faith based.” [As if ‘the way it’s always been’ is a sound argument for ‘the way it always should be.’ Perhaps we shouldn’t have moved from serfdom to democracy?]
“The Catholic Church began the medieval hospice movement, and can lead the modern palliative care movement.” [They curiously neglect to mention that the palliative care (not hospice) movement rose from Anglican roots in the UK, helpfully confirming that this broadcast is primarily about promoting Catholic religion, not palliative care.]
Shameless self-promotion
But Dr Pettus and the IAHPC’s Concept Note don’t stop there.
“The Word [sic] Day of the Sick (WDS) is a good opportunity to support faith based healthcare organizations.”
“Contact your parish to see if you can hold a small event…”
“Contact your local Catholic health care provider director to find out about…”
“Make an announcement at your local church…”
Gosh, I must have been mistaken. I thought World Day of the Sick was about… the sick!?
But Dr Pettus and the IAHPC commandeer it to shamelessly further the Catholic religious agenda amongst palliative care service providers.
An unexamined conflict of interest
It's deeply disturbing that someone holding the position of “Advocacy and Human Rights Officer” considers the beliefs and values only of the service provider (who she represents) in promoting the world day about sick people (who her organisation serves).
Palliative care organisations repeatedly state that they aim to deliver patient-centred care. But the world palliative care peak body's self-adoration exposes the worst of them: taking the opportunity of a day supposedly for the values and needs of sick patients, and using it to glorify their own particular (Catholic) religious tenets which are to be lauded over those of the patients they serve.
Most of the world is not Catholic, and in Australia at least, most Catholics disagree with Vatican doctrine on assisted dying.
How astonishing then to dictate that Catholic doctrine must prevail over everyone, including Protestants, Hindus, Buddhists, Jews, Muslims, agnostics, atheists and others. Dr Pettus and the IAHPC comprehensively fail to demonstrate any awareness or reflection of potential conflicts of interest in serving people of different faiths and beliefs.
Incomprehensible arrogance
There is little issue with the Catholic Church directing its own willing adherents as to how they might end their days.
But for one religious institution to seek to impose its views on everyone worldwide is incomprehensibly arrogant. I guess it's no surprise then that a Catholic Bishop recently admitted — at a Royal Commission inquiry into the extensive, ongoing and horrific abuse of children under the Church's pastoral care — that the Catholic Church is a "law unto itself".
It would be helpful if the Holy See reflected on the principle: is it legitimate for another faith to force its own views on the Vatican or on Catholic patients?
It would also be helpful if the International Association of Hopsice and Palliative Care reflected on respecting and serving the wider community rather than behaving like a subsidiary of the Holy See.
Conclusion
The IAHPC has provided its own unequivocal proof that it is religious conservatism behind organised opposition to assisted dying, with the Catholic Church at the front of the pack.
You’ll understand why I tweeted in response to Dr Pettus:
“.@kpettus @EAPCOnlus Thanks for confirming @Pontifex arrogance. Not once did you mention PATIENT’S PoV. All about YOU.” — Neil Francis
- - -
And furthermore
Parading ignorance
The IAHPC refers repeatedly to the treatment of ‘pain’ in its stand against assisted dying law reform. But pain is not amongst the leading reasons for assisted dying (it is a much less common reason). Key reasons are the inability to participate in any of life’s enjoyable activities, loss of independence and loss of dignity.
I guess the curious focus on ‘pain’ is understandable though, because the Vatican is very fond of the doctrine of double effect (DDE) — which the IAHPC specifically notes in Catholic Catechism 2279 although not by its DDE name, but rather bizarrely as “a special form of disinterested charity.”
The DDE posits that it’s OK for a doctor to administer high doses of analgesics to treat pain, even if an unintended consequence is to hasten the patient’s death. The Catholic Church treats this doctrine as uncontroversial, even though it remains controversial amongst other ethicists and philosophers: the principle says “it’s quite OK for a doctor to kill her patient, as long as she doesn’t really mean to.”
I would commend Dr Pettus and the IAHPC to do some proper research and understand the subject area more competently before pontificating (yes, intended meaning) further.
The smokescreen argument
The IAHPC also states that:
“No country or state should consider the legalization of euthanasia or PAS until it ensures universal access to palliative care services.”
That’s purely a smokescreen argument for two reasons. Firstly, the Concept Note also argues that assisted dying:
“both violate[s] the bond of trust within the profession of medicine, and undermine[s] the integrity of the profession and the dedication to safeguard human life.”
Setting aside the empirical falsehood of the statement, it furnishes the IAHPC a 'get-out-of-jail-free' card if and when palliative care becomes ‘universally’ available: it’s utterly irrelevant if that goal is reached because there’s a more fundamental objection behind it.
Secondly, it's an established fact that palliative care can’t always help, even when the best services are available. ‘Universal’ access won’t fix all the problems.
All these faux arguments are typical and common from religious opponents of assisted dying.
Fact file by Neil FrancisPosted on Sunday 13th November 2016 at 1:47am
Assisted dying rates in Dutch-speaking cultures (orange bars) are much higher than elsewhere.
In this whitepaper, Benelux (Belgium, Netherlands and Luxembourg) primary empirical data on assisted dying is analysed — including with new and advanced approaches — to provide fresh insights into contemporary practices. Investigation reveals that the assisted dying rate in Dutch-speaking cultures appears to be uniquely higher than in other cultures irrespective of the permissiveness of the legislative framework, yet is still practiced conservatively.
Download a full copy of the Whitepaper here: PDF (648Kb).
Summary
This new compilation and unique analysis of primary research data from statutory authorities and the peer-reviewed literature provides fresh insights into assisted dying practice in Benelux, including:
Rates of assisted dying in the Netherlands and Belgium have followed an expected sigmoid curve, now beginning to level out.
Several factors have contributed to the higher increase in the Netherlands rate, including recovery from a suppression of cases immediately following statutory reform, a rise in cancer diagnoses, and an increase in granting of assisted dying through new visiting teams launched in 2012.
Both Netherlands and Belgium doctors demonstrate caution if not conservatism when assessing assisted dying requests.
Despite most assisted dying occurring in cases of cancer, fewer than one in ten cancer deaths in the Netherlands and one in twenty in Belgium is an assisted death.
Other conditions such as degenerative neurological, pulmonary and circulatory illnesses each account for a very small proportion of the increase in cases since legalisation in Benelux.
The assisted dying rate in dementia and other mental illness is very low despite controversy around—and a tiny rise in granting of—such cases.
The hypothesis that females or the elderly would be ‘vulnerable’ to assisted dying law is contradicted by the data.
The rate of non-voluntary euthanasia has decreased significantly in both the Netherlands and Belgium since assisted dying was permitted by statute.
Assisted dying rates in Dutch-speaking cultures are significantly higher than in non-Dutch cultures, seemingly unrelated to the permissiveness of the jurisdiction’s legal framework.
Benelux country reported assisted dying rates (as a percentage of all deaths)
as at 2014. The three countries have similar assisted dying laws.
Blog by Neil FrancisPosted on Sunday 28th August 2016 at 12:58am
Brad Mattes' blog containing misleading and evidentially false statements.
The latest misinformation employed by assisted dying opponents is to imply that Belgium’s general suicide rate is high as a consequence of its assisted dying law: i.e. to argue the discredited 'suicide contagion' line which has in the past been peddled about the USA state of Oregon. I have demonstrated that it was false in Oregon, and I equally demonstrate here that it's false in Belgium.
Mr Brad Mattes recently published emotional anti-assisted-dying nonsense in LifeSiteNews. (LifeSiteNews is a Canadian blog site that was established by the conservative Christian Campaign for Life Coalition and which has a primary principle of promoting “traditional Judeo-Christian principles”. Mr Mattes is radio host for Ohio’s Life Issues Institute, an anti-abortion lobby group established by conservative American John C. Willke who claimed that women’s bodies were resistant to pregnancy as a result of rape.)
Putting on the misinformation running shoes
In his blog Mr Mattes quickly establishes a practice of communicating misinformation by first claiming that assisted dying laws have “devastating effects” around the world including Japan and Albania—which don’t have such laws.
He then sprints onwards to the ‘650 babies euthanized in the Netherlands’ claim—which I have already comprehensively exposed as fake in the Journal of Assisted Dying—and then onto the bogus claim that the Netherlands has descended into a mire of ‘killing’ without the patient’s ‘consent,’ contrary to empirical evidence I've published that such actions occur around the world regardless of assisted dying laws, and which have decreased significantly in the Netherlands and Belgium since their assisted dying statutes came into effect in 2002.
Let’s add fries to that
Having served up a lot of fat and salt that might appeal to those on a fast-food anti-assisted-dying diet, he then offers the unqualified statement:
“By the way, Belgium has the second-highest suicide rate (nonrelated to euthanasia) in Western Europe.” — Brad Mattes
The ‘informational’ consequence is unequivocal: by Mr Mattes failing to contextualise this ‘incidental factoid’ in any way, the reader is destined to deduce that it is Belgium’s euthanasia law that causes Belgium’s suicide rate to be the second-highest in Western Europe. In other words, Mr Mattes is another poorly-informed commentator using the 'suicide contagion' line.
But what are the facts?
Depending on the source and year of data, one can certainly argue that Belgium’s general suicide rate is the second-highest in Western Europe. Setting aside for now the serious question of why it is valid to exclude all of the world’s other countries from the comparison, WorldLifeExpectancy.com reports figures that were published in 2014 (Table 1).
Table 1
Country
Suicides*
Finland
15.11
Belgium
14.64
Iceland
14.06
France
12.84
Austria
11.87
Sweden
11.43
Ireland
11.06
Germany
9.59
Switzerland
9.56
Norway
9.28
Denmark
9.19
Luxembourg
9.14
Netherlands
8.54
Portugal
8.49
Turkey
7.92
UK
6.28
Malta
5.75
Spain
5.23
Italy
4.76
Greece
3.86
* Suicides per 100k population, age-adjusted
The table includes all the countries in the wider definition of “Western Europe”, bar four: no suicide statistics are published for Liechtenstein, Monaco, Andorra or San Marino.
As you can see, Belgium is indeed the second-highest. But this begs the question:
If the reason Belgium is the second-highest is due to its assisted dying law, how come Finland, which Mr Mattes doesn't mention by name and which has no such law, is higher?
It also begs the question:
If assisted dying law were the fundamental cause of a high general suicide rate, how come Switzerland (statute since 1942), Luxembourg (statute since 2009) and the Netherlands (practice since the early 1980s and statute since 2002) have rates that are muchlower, all key facts that Mr Mattes also fails to mention?
These are of course indications that the factoid has been included as a cherry-picked morsel of 'proof' because it sounds so compelling as a throw-away sentence amongst the other (false) statements.
But wait, there’s more
We can go further than merely wondering about the country comparisons, by comparing Belgium’s general suicide rate before and after assisted dying law reform. A critical step in establishing causation is to first establish correlation. If there is no correlation, there can be no causation.
Published OECD data shows that in 2013 (the most recent available data), Belgium’s general suicide rate was 16.7 per 100,000 population. What was it before their 2002 law reform? Well in 2000 it was 20.5, in 1990 it was 19.2, … you get the idea.
Has Belgium’s general suicide rate soared (or even increased modestly) since their 2002 assisted dying law came into effect? No. It’s dropped. Indeed, the slight downward trend apparent before the statute came into effect in 2002 has accelerated downward since (Figure 1).
Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Even the headline is misleading
Mr Mattes fails to point out in his blog that assisted dying statutes in Benelux countries (Belgium, the Netherlands and Luxembourg) never restricted access to only the 'terminally ill,' that is, those imminently dying. He also fails to point out that USA states whose laws do restrict assisted dying to the terminally ill—most notably Oregon and Washington—have not changed their statutes in this regard since they came into effect.
Therefore, his headling implying that lawful jurisdictions have broadened their laws from 'only the terminally ill' is also wrong.
Conclusion
Mr Mattes makes multiple false and misleading claims and it’s easy to see his opinion for what it is: an emotional dump that fails to engage with and indeed flies in the face of actual evidence. The latest 'suicide contagion' implication, that assisted dying law causes Belgium’s general suicide rate to be the “second-highest in Western Europe” is evidentially false.
I call on LifeSiteNews to withdraw Mr Mattes' article because it breaches their primary principle:
“1. Accuracy in content is given high priority. News and information tips from readers are encouraged and validated. Valid corrections are always welcome. Writing and research is of a professional calibre.” — LifeSiteNews
Summary of facts
Belgium's general suicide rate is one of the higher ones in Western Europe. However:
At least one country without an assisted dying law has a higher suicide rate, inconsistent with 'suicide contagion' theory.
Other Western Europe countries with assisted dying laws have suicide rates much lower than Belgium's, also at odds with 'suicide contagion' theory.
But the clincher is that the suicide rate in Belgium has dropped, not risen, since their 2002 assisted dying law came into effect.
The F filesPosted on Monday 8th August 2016 at 7:02am
Back in 2013 the High Court of Ireland rejected a legal bid by multiple sclerosis sufferer Marie Fleming to achieve a lawfully-assisted peaceful death.
The Court naturally relied on expert testimony in reaching its judgement, yet its conclusions included a statement containing significant errors of fact.
The erroneous statement
In its judgement,1 the Court made the following statement:
“Above all, the fact that the number of LAWER (“legally assisted deaths without explicit request”) cases remains strikingly high in jurisdictions which have liberalised their law on assisted suicide (Switzerland, Netherlands and Belgium) — ranging from 0.4% to over 1% of all deaths in these jurisdictions according to the latest figures — without any obvious official response speaks for itself as to the risks involved.” [My emphases in bold]
In fact, the Court's judgement is wrong on not one, not two, but three significant matters. But that hasn't stopped opponents of assisted dying law reform from quoting the judgement as though it were factual and persuasive, when it isn't: relying on it because it was made by a High Court—the 'authority bias.'
Consequences
Here are just a few examples of the Court's statement being wielded by assisted dying opponents as though it were conclusive evidence against law reform:
Family First’s submission opposing assisted dying law reform in New Zealand.
Catholic lobbyist Paul Russell and Catholic NSW MP Greg Donnelly in submissions to the Victorian (Australia) Parliament inquiry into end-of-life choices.
Catholic Professor Margaret Somerville in the New England Journal of Medicine,2 repeated by Alex Schadenberg of the Euthanasia Prevention Coalition as well as by Catholic-founded National Right To Life News; and Somerville again in the (Catholic) Newman Rambler.3
These examples illustrate the frequency of quoting the misinformation and how it feeds into and wrongly shapes public policy formation.
Three strikes
So what are the three counts on which the Court's judgement was seriously wrong?
Strike 1: Wrong concept
First, let’s get the concepts right. LAWER is not “legally assisted deaths without explicit request.”
Such nomenclature is an oxymoron. To ‘assist’ is to accommodate, serve or help someone accomplish something. But if there has been no request then one cannot be helping. You can’t ‘assist’ a little old lady across the road if she has expressed no interest in going there: you’d be forcing her across the road. Equally, you can’t ‘assist’ a death if there’s no proper ‘request.’
LAWER in fact stands for “Life-ending Acts Without Explicit Request” (of a competent patient).5 And with the exception of the possible ‘lawfulness’ of the doctrine of double effect, such acts are illegal.
Further, if such acts were legal as the Court’s statement posits, then there would be no need for an “obvious official response” as the Court then concludes. The statement lacks fundamental coherence.
Strike 2: Not ‘strikingly high’
The Court's judgement states unequivocally that LAWER (otherwise known as Non-Voluntary Euthanasia or NVE) rates in Switzerland, the Netherlands and Belgium are ‘strikingly high’, though no comparative yardstick is recorded in the judgement by which one might draw or justify that subjective judgement. Similar 'strikingly high' statements also appear in sections 102 and 104 of the judgement.
There is in fact a scientific study, published in The Lancet in 2003, that provides sound empirical evidence that could have properly informed the Court (Figure 1).6
Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002
As revealed by this study, the NVE rates in Switzerland and the Netherlands were in fact lower than in Denmark, a country which has never had an assisted dying law.
The only country which did appear to have an NVE rate notably higher than the others was Belgium. The research study collected the data for analysis between June 2001 and February 2002. However, Belgium’s Euthanasia Act was not passed by its Parliament until 28th May 2002, well after data collection was complete. Thus, even in describing Belgium’s NVE rate as ‘strikingly high’ compared to a number of other European countries, it cannot be attributed to an assisted dying law because none existed at the time.
In fact, the NVE rate in Belgium had been found to be high back in 1998,7 well before the Bill for the country's Euthanasia Act was even tabled in Parliament.
Further, if assisted dying laws had such effects, it might be expected that the NVE rate would increase the longer that assisted dying laws were in place. In that case the NVE rates in Switzerland (statute since 1942) and the Netherlands (regulation since the early 1980s) would have NVE rates much higher than Belgium’s (statute since 2002). But the exact opposite is true.
Indeed, Rietjens and colleagues8 further concluded in their review of NVE in the Netherlands, Belgium, Denmark and Switzerland that “the use of drugs with the intention to hasten death without an explicit request of the patient is part of medical end-of-life practice in the studied countries, regardless of their legal framework, and it occurs in similar fashion.” The study, published in 2007, would also have been important evidence before the Court.
Strike 3: Not ‘remaining’ high
The Court's judgement states unequivocally that the LAWER (NVE) rate of the three countries ‘remains’ strikingly high. No specific evidence was supplied in the judgement to support this statement. Indeed, the judgement notes:
In section 28 that Dutch NVE had been “consistently declining.”
In section 91 that “the number of LAWER deaths has significantly declined in both [Dutch and Belgian] jurisdictions.”
In section 94 that “the trend in [Dutch] LAWER cases are declining in numbers (from 1,000 in 1990 to 550 in 2005)” and that in Belgium “the number of LAWER cases has declined since legalisation of assisted death.”
In section 101 that the NVE rates of both the Netherlands and Belgium had dropped.
Despite this clear and repeated evidence, the Court summarises in section 96 that the evidence cannot be “regarded as encouraging or satisfactory.”
But what does empirical research tell us about the NVE trends? In both the Netherlands and Belgium, since assisted dying was enshrined in statute and became effective in 2002, the rate of NVE has decreased significantly (Figure 2).7,9-11 In fact, the rate in the Netherlands is now similar to that in the UK, a country which has never had an assisted dying law and which provides the world’s gold standard in palliative care practice.
Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying
These are critical yardsticks by which to judge practice in jurisdictions that have assisted dying laws with jurisdictions that don't. The UK study was published in 2009 and was readily available prior to the High Court’s hearings, yet appears not to have been presented in evidence.
The final (2010) Dutch NVE statistic in Figure 2 may or may not have been available to the Court: it was published in 2012 around the time the Court was taking evidence. The final (2013) Belgian statistic would not have been available to the Court as it was published in 2015.
Conclusion
While the High Court worked diligently within the scope of evidence brought before it:
The Court’s definition of LAWER is incorrect and incoherent;
Its statement that the NVE rates of the Netherlands and Switzerland are ‘strikingly high’ are evidentially wrong when compared with other countries without assisted dying laws;
Its implication that the higher NVE rate in Belgium was caused by assisted dying law reform is evidentially wrong; and
Its statement that the rates remain high is evidentially wrong.
The High Court's judgement does not provide defensible evidence or argument against assisted dying law reform.
Many lobbyists have repeated these incorrect statements, significantly misleading media, policy makers and legislators.
Now that the facts are readily available it’s appropriate to avoid repeating evidentially wrong statements, regardless of the apparent 'authority' of their source.
Summary of facts
LAWER stands for "Life-ending Acts Without Explicit Request". Its practice is similar in countries with and without assisted dying laws.
The NVE rates in the Netherlands and Switzerland are lower than the rate in Denmark, a country which has never had an assisted dying law.
The NVE rate in Belgium appears higher, but was so long before assisted dying law reform and so cannot have been caused by such a law.
The NVE rates of the Netherlands and Belgium have both decreased significantly since their assisted dying statutes came into effect in 2002.
References
High Court of Ireland 2013, Fleming v Ireland & Ors - Determination, [2013] IEHC 2, Dublin.
Boudreau, JD, Somerville, MA & Biller-Andorno, N 2013, 'Physician-assisted suicide: should not be permitted/should be permitted', New England Journal of Medicine, 368(15), pp. 1450-1452.
Somerville, M 2016, 'Killing as kindness: The problem of dealing with suffering and death in a secular society', The Newman Rambler, 12(1), pp. 1-26.
Keown, J 2014, 'A right to voluntary euthanasia? Confusion in Canada in Carter', Notre Dame Journal of Law, Ethics & Public Policy, 28(1), pp. 1-45.
Pijnenborg, L, van der Maas, PJ, van Delden, JJM & Looman, CW 1993, 'Life-terminating acts without explicit request of patient', Lancet, 341(8854), pp. 1196-1199.
van der Heide, A, Deliens, L, Faisst, K, Nilstun, T, Norup, M, Paci, E, van der Wal, G & van der Maas, PJ 2003, 'End-of-life decision-making in six European countries: descriptive study', The Lancet, 362(9381), pp. 345-350.
Bilsen, J, Cohen, J, Chambaere, K, Pousset, G, Onwuteaka-Philipsen, BD, Mortier, F & Deliens, L 2009, 'Medical end-of-life practices under the euthanasia law in Belgium', New England Journal of Medicine, 361(11), pp. 1119-1121.
Rietjens, JA, Bilsen, J, Fischer, S, Van Der Heide, A, Van Der Maas, PJ, Miccinessi, G, Norup, M, Onwuteaka-Philipsen, BD, Vrakking, AM & Van Der Wal, G 2007, 'Using drugs to end life without an explicit request of the patient', Death Studies, 31(3), Mar, pp. 205-21.
Seale, C 2009, 'End-of-life decisions in the UK involving medical practitioners', Palliat Med, 23(3), pp. 198-204.
Onwuteaka-Philipsen, BD, Brinkman-Stoppelenburg, A, Penning, C, de Jong-Krul, GJF, van Delden, JJM & van der Heide, A 2012, 'Trends in end-of-life practices before and after the enactment of the euthanasia law in the Netherlands from 1990 to 2010: a repeated cross-sectional survey', The Lancet, 380(9845), pp. 908-915.
Chambaere, K, Vander Stichele, R, Mortier, F, Cohen, J & Deliens, L 2015, 'Recent trends in euthanasia and other end-of-life practices in Belgium', N Engl J Med, 372(12), pp. 1179-1181.

 The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.
The Catholic Church approves of the theoretical risk of the left-hand course (refusal of life-saving medical treatment), but not of the theoretical risk of the right-hand course (assisted dying) which is lower in practice by virtue of considerably more statutory safeguards.

 Figure 1: ICU was used in the last 30 days of life
Figure 1: ICU was used in the last 30 days of life Figure 2: Patient was discharged from hospital in the last 30 days of life
Figure 2: Patient was discharged from hospital in the last 30 days of life Figure 3: Dying patient received hospice care at home
Figure 3: Dying patient received hospice care at home Figure 4: The individual died at home
Figure 4: The individual died at home

 “#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
“#Catholic church @Pontifex believes all life is sacred&supports #PalliativeCare and use of strong #pain medicines” — Dr Katherine Pettus
 Figure 1: The Belgium general suicide rate before and after assisted dying law reform
Figure 1: The Belgium general suicide rate before and after assisted dying law reform Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002
Figure 1: The non-voluntary euthanasia (NVE) rates of seven European countries in late 2001/early 2002 Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying
Figure 2: Empirical trends in NVE rates before and after legalisation of assisted dying